maging the Pancreas – Plain Film
Author Ashley Davidoff MD
Collaborators Charles Allison MD Adam Asarch MSII David Lee MD Scott Tsai MD Sam Yam PhD.
The plain film does not have much role in the diagnosis of acute pancreatitis. there are occasional findings that are helpful, but these are in general not common nor specific.
Acute Pancreatitis – Colon Cut-off Sign
 This plain film of the abdomen shows a colon cut-off sign at the splenic flexure. The left colon and the splenic flexure more specifically, are common targets for dissecting enzymes which cause inflammation and spasm of the colon. 04922 Courtesy Ashley Davidoff MD
This plain film of the abdomen shows a colon cut-off sign at the splenic flexure. The left colon and the splenic flexure more specifically, are common targets for dissecting enzymes which cause inflammation and spasm of the colon. 04922 Courtesy Ashley Davidoff MD
 This plain film of the abdomen shows a colon cut-off sign at the splenic flexure. The left colon and the splenic flexure more specifically, are common targets for dissecting enzymes which cause inflammation and spasm of the colon. 41543 Courtesy Ashley Davidoff MDchronic pancreatitis
This plain film of the abdomen shows a colon cut-off sign at the splenic flexure. The left colon and the splenic flexure more specifically, are common targets for dissecting enzymes which cause inflammation and spasm of the colon. 41543 Courtesy Ashley Davidoff MDchronic pancreatitis
Subacute Pancreatitis – Pseudocyst formation
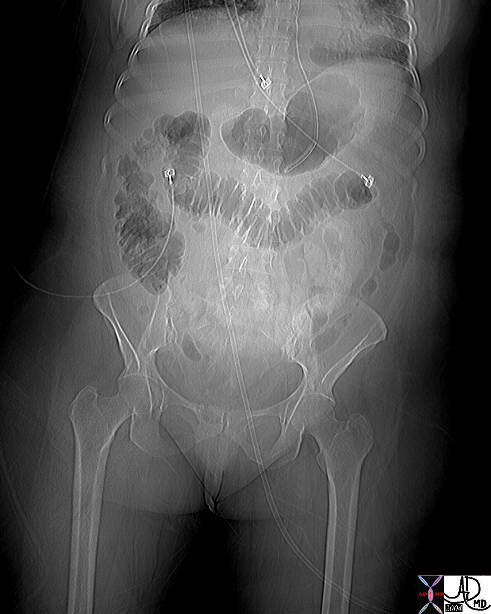
 This plain film of the abdomen is from a patient who had had an episode of acute pancreatitis 6 weeks prior and presented with abdominal pain and distension. The mass effect on the superior aspect of the colon is caused by a large pseudocyst. Courtesy AshleyDavidoff MD. 40280
This plain film of the abdomen is from a patient who had had an episode of acute pancreatitis 6 weeks prior and presented with abdominal pain and distension. The mass effect on the superior aspect of the colon is caused by a large pseudocyst. Courtesy AshleyDavidoff MD. 40280
Calcification of thre pancreas is almost pathognomonic for alcoholic pancreatitis, but has been seen in patients with congenital cysts, pancreatitis secondary to Crohn’s disease. Thius finding calcificatoin in the position and shape of the pancreas on a plain film, is almost pathognomonoc with alcoholic pancreatitis.
Chronic Pancreatitis
 This plain film of the abdomen shows the tubular shaped calcification of the pancreas which lies in the transpyloric plane. Incidental finding is a compression screw in the right hip. The most common and likely diagnosis is chronic pancreatitis 32913 Courtesy Ashley Davidoff MD
This plain film of the abdomen shows the tubular shaped calcification of the pancreas which lies in the transpyloric plane. Incidental finding is a compression screw in the right hip. The most common and likely diagnosis is chronic pancreatitis 32913 Courtesy Ashley Davidoff MD
 The patient above also had a lateral examination which shows the relative posterior and high position of the tail, and the inferior and anterior position of the uncinate process. Incidental findings include the calcified atherosclerotic abdominal aorta and the degenerative changes at L3-L4. 32916 Courtesy Ashley Davidoff MD
The patient above also had a lateral examination which shows the relative posterior and high position of the tail, and the inferior and anterior position of the uncinate process. Incidental findings include the calcified atherosclerotic abdominal aorta and the degenerative changes at L3-L4. 32916 Courtesy Ashley Davidoff MD