The Common Vein Copyright 2008
Definition
Acute pancreatitis is an acute inflammatory condition of the pancreas usually caused by the toxic effect of an acute alcoholic binge or displaced gallstones, resulting in varying degrees of local and regional damage. In 80-90% of cases the inflammation is contained and the damage is reversible. If there is duct injury and spillage of digestive enzymes there is a varying degree of autodigestion and destruction of the tissues. The fact that the pancreas has no capsule is an important deficiency and allows for the enzymes that are released to be given free reign of destruction in the anterior pararenal space of the retroperitoneum. Given the opportunity the enzymes show no mercy on any tissue in their path. They declare chemical warfare on any fat, or collagen . They wreak havoc by moving beyond the retroperitoneum and destroying tissues in almost any location in the abdomen and sometimes beyond.
The diagnosis is suspected clinically by the abdominal pain and back pain that occur and is confirmed bty elevated levels of serum amylase and lipase. CTscanning is the imaging study of choice to identify the severity of the disease and to evaluate for complications.
Treatment is usually conservative with specific attention to volume replacement and pain management. When complicated by abscess or necrosis, surgical debridement is indicated.
Pathology
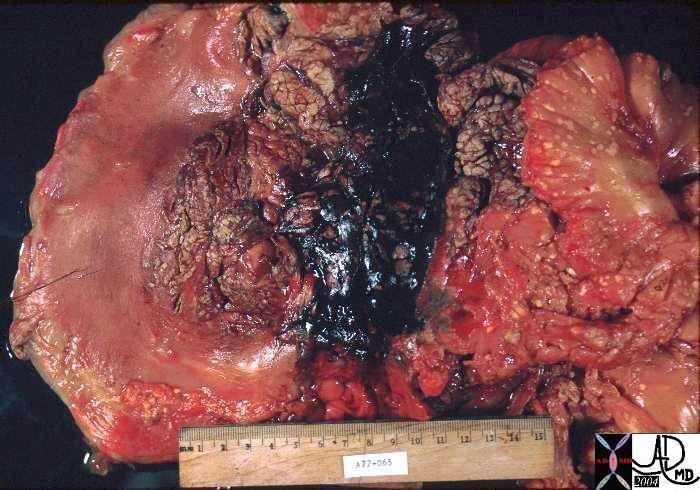 Pancreatic Hemorrhage Pancreatic Hemorrhage |
| This gross pathology specimen shows the swollen tissues lying in the c sweep of the duodenum. A hemorrhagic component overlies the neck of the pancreas.15289 Courtesy Barbara Banner MD |
The size of the gland is slightly increased but the main changes occur in the surrounding tissues. The gland softens in areas of necrosis and may be discolored particularly when hemorrhage has occurred. Gray-white areas of necrosis are intermingled with black and blue bruising of the hemorrhagic areas. The surrounding fat undergoes saponification and calcification becoming a yellow-white in color and chalky in texture
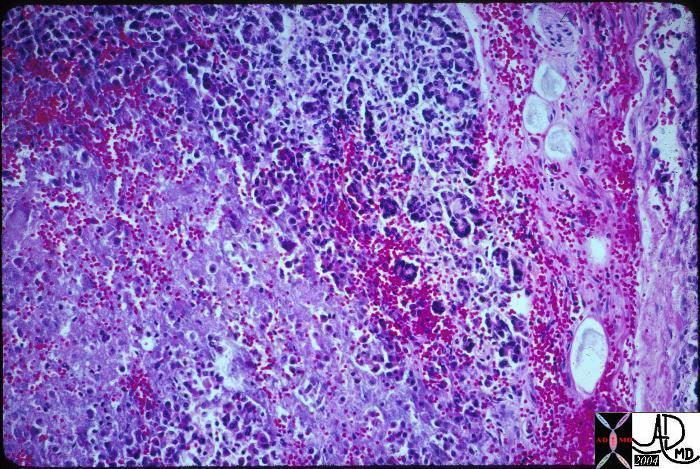 Pancreatitis Pancreatitis |
| This histopathology section shows a combination of hemorrhage necrosis and cellular infiltrate in this specimen with acute pancreatitis 15286 Courtesy Barbara Banner MD |
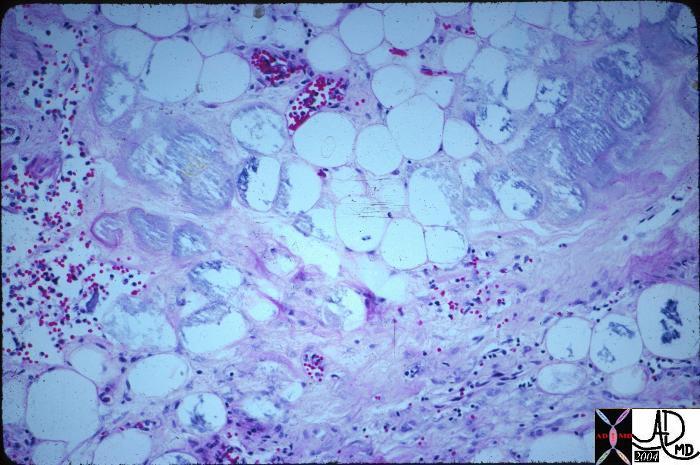 Pancreatitis Pancreatitis |
| This histopathology section shows a necrosis and cellular infiltrate in this specimen with acute pancreatitis 15283 Courtesy Barbara Banner MD |
Imaging Approach
We have divided the imaging atlas of acute pancreatitis into the acute form of the disease (within hours of presentation), subacute form (within days or weeks), and the complications of the disease that occur within weeks. Chronic pancreatitis has been reserved for the changes of the pancreas that occur over the years.
In the acute phase the phlegmon is characterized by exudative fluid in and around the pancreas. If there is damage to the blood vessels in the more severe form, hemorrhagic change occurs and this entity is of course known as hemorrhagic pancreatitis, recognized by high density within the pancreas on examination with CTscan. In this section we will also show uncommon examples including traumatic pancreatitis and infections.
The acute imaging presentation is characterized mostly by phlegmonous changes around the pancreas with spread around the anterior pararenal space in the mild forms and extension of beyond into the mesentery of the abdomen and peritoneum in the more severe cases.The diagnosis of acute pancreatitis is usually easily made on clinical grounds, and the object of imaging is to determine the morphological damage as a result. Since the disease once launched is like a smoldering gun. It has acute effectsto consider, and subacute effects if not contained. In both instances CT is the study of choice due to its global ability to easily and with great resolution, evaluates the retroperitoneum, peritoneal cavity and pelvis.
Inthe acute stages the procedure requires a non contrast study first in order to distinguish between a phlegmonous pancreatitis and a hemorrhagic pancreatitis. The noncontrast study is also used to identify calcifications – footprints of previous disease. A contrast study in portal venous stage should me performed next, unless pancreatic necrosis is suspected in which case an arterial phase should also be performed. In the early stages of the disease, the degree of pancreatic exudate and the extent to which it has spread are the important decisions to be made. Understanding the retroperitoneal anatomy is key to this evaluation. The process may be confined to the retroperitoneal space in less severe forms, but with advancing disease it may spread laterally into the flanks, inferiorly to the groin or superiorly to the subdiaphragmatic position. The spreading process may affect the abutting organs of the retroperitoneum such as the colon pleura and kidneys and vessels. If the disease is more aggressive it may break out from the anterior pararenal space into the peritoneal cavity anteriorly or through the properitoneal fat plane laterally and into the subcutaneous tissues. If the patient dos not recover follow up imaging to assess ongoing morphological damage of saponification of fat, pseudocyst formation, pancreatic necrosis, infection, splenic thrombosis, and pseudoaneurysm is essential. Most of these complications can be clinically but very obvious on imaging.

Pancreas |
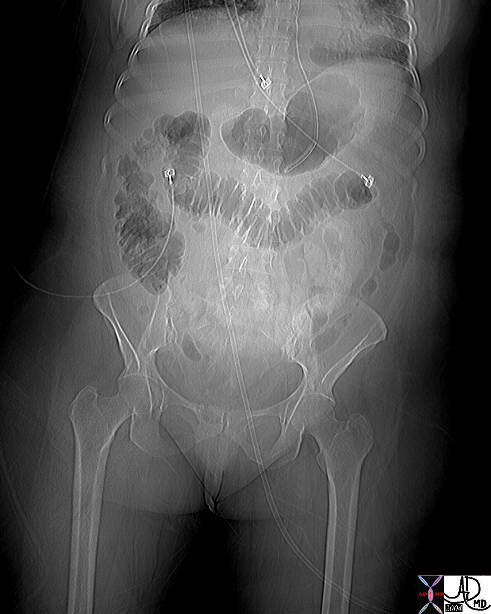
| This plain film of the abdomen shows a colon cut-off sign at the splenic flexure. The left colon and the splenic flexure more specifically, are common targets for dissecting enzymes which cause inflammation and spasm of the colon. 04922 Courtesy Ashley Davidoff MD |
Pancreas |
| This plain film of the abdomen shows a colon cut-off sign at the splenic flexure. The left colon and the splenic flexure more specifically, are common targets for dissecting enzymes which cause inflammation and spasm of the colon. 41543 Courtesy Ashley Davidoff MD |
Pancreas |
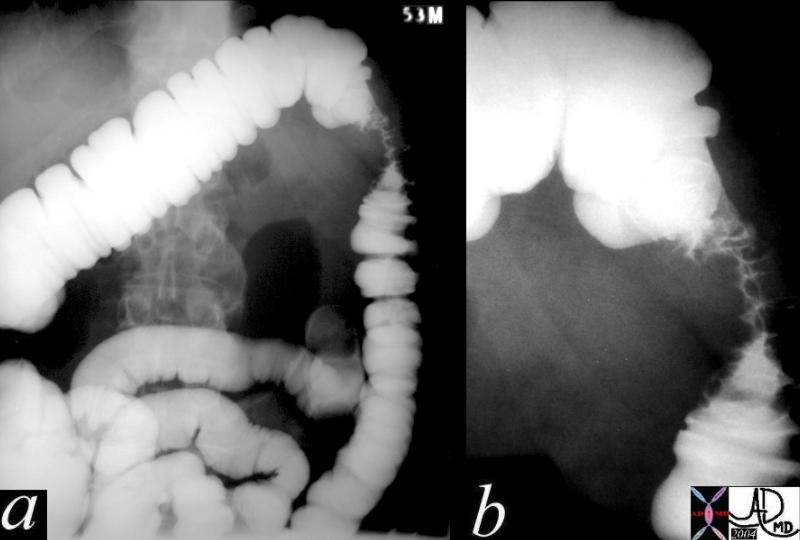
| This barium enema of a 53 year man with pancreatitis shows focal spasm of the splenic flexure caused by spreading exudate along the lleft lateral aspect of the anterior pararenal space to the paracolic gutter. 40310c Courtesy Ashley Davidoff MD |
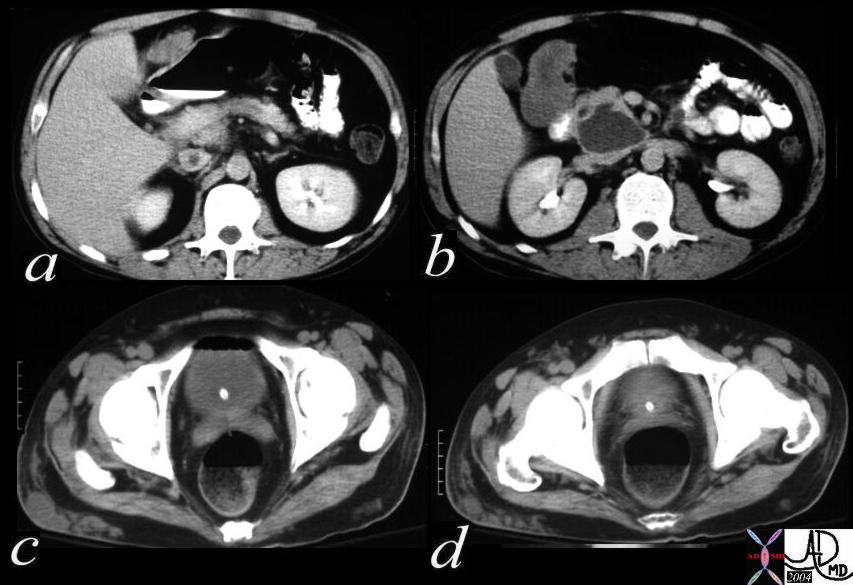
Pancreas |
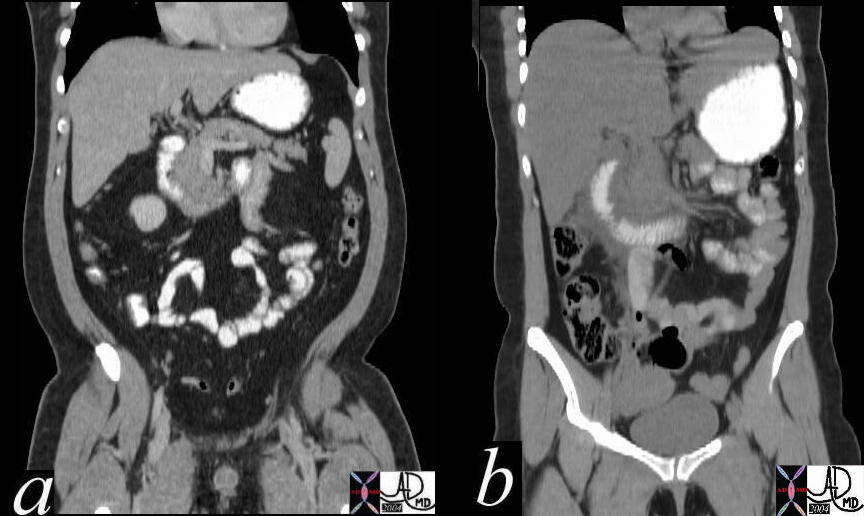
| This combination of coronally reformatted images of the abdomen show a normal c- sweep in a, and an enlarged and widened c-sweep in b. The patient in b, had acute pancreatitis with swelling of the pancreatic head caused mostly by the exudate which is seen on either side of the duodenum. 40999c02 Courtesy Ashley Davidoff MD |
Acute Pancreatitis The Phlegmon

Pancreas |
| This CT scan through the pancreas shows a relatively normal sized pancreas with a large peripancreatic effusion. (phlegmon) This type of change is characteristic of phlegmonous pancreatitis The absence of a pancreatic capsule allows free leakage of the exudative component of the inflammation out of the pancreas and into the anterior pararenal space. Note there is involvement of the lateral conal fascia on the left, thickening of the peritoneum (implying transgression of the properitoneal fat line), and soft tissue changes in the hypodermis. The latter finding if hemorrhagic is the radiologic equivalent of the Gray-Turners sign. 15730 Courtesy Ashley Davidoff MD |

Pancreas |
| This angiogram is from a prior era of pancreatic imaging, and it is used to demonstrate the mild swelling of the pancreas in a 50 year old female with acute abdominal pain, elevated amylase and a diagnosis of acute pancreatitis. 40918 Courtesy Laura Feldman MD |
When the acute pancreatitis is more severe it path of destruction extends beyond the retroperitoneum and into the peritoneal cavity. It may spread along the mesentery or break directly through the posterior parietal peritoneum which forms its anterior border.
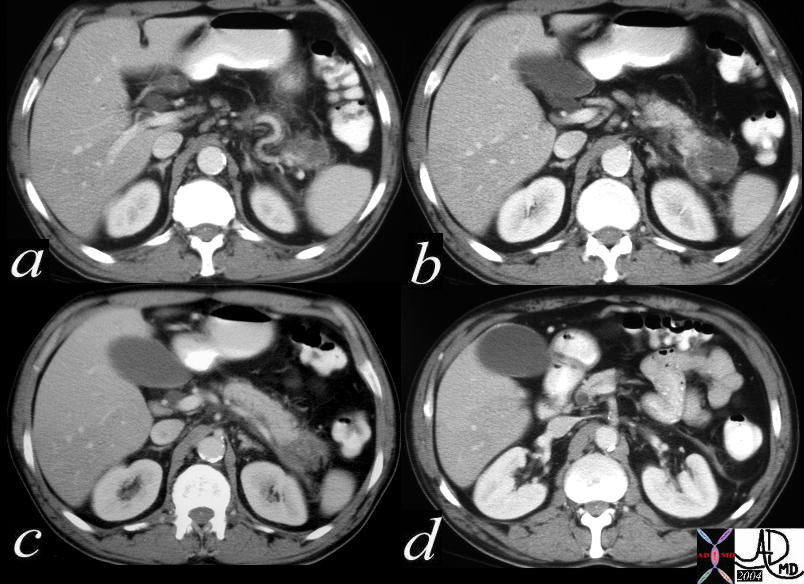
Pancreas |
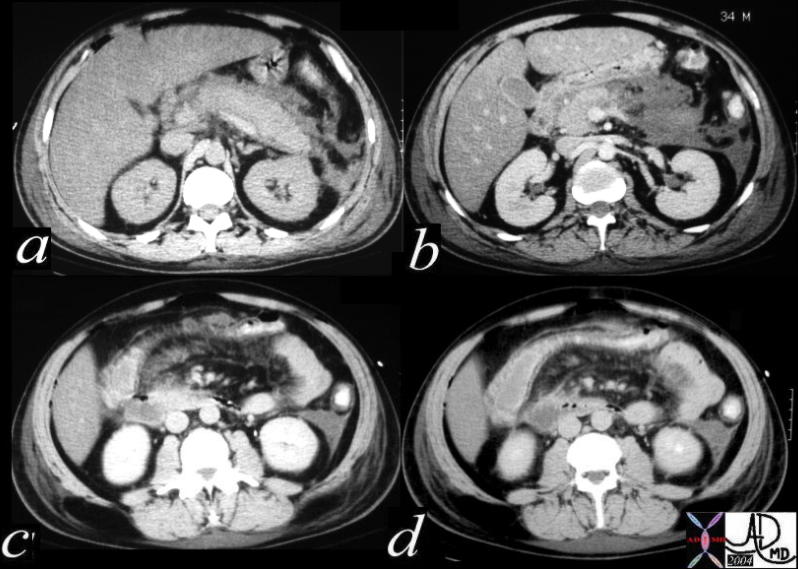
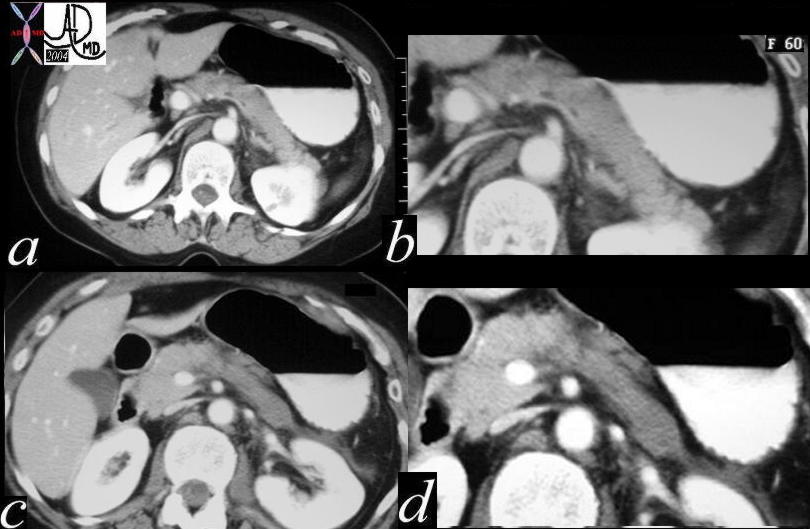
| This is the case of a 34 year old male with acute pancreatitis following and alcoholic binge. In this combination of CT images through the abdomen, the findings are characterized by a peripancreatic exudate (a) which extends to the left paracolic gutter via Gerota’s fascia and lateral conal fascia (b). The path of destruction extends into the base of the transverse mesocolon in c, causing thickening of the serosa of the transverse colon (d). 40215c Courtesy Ashley Davidoff MD |
In the images that follow we single out the spread of the process along the transverse mesocolon.
Pancreas |
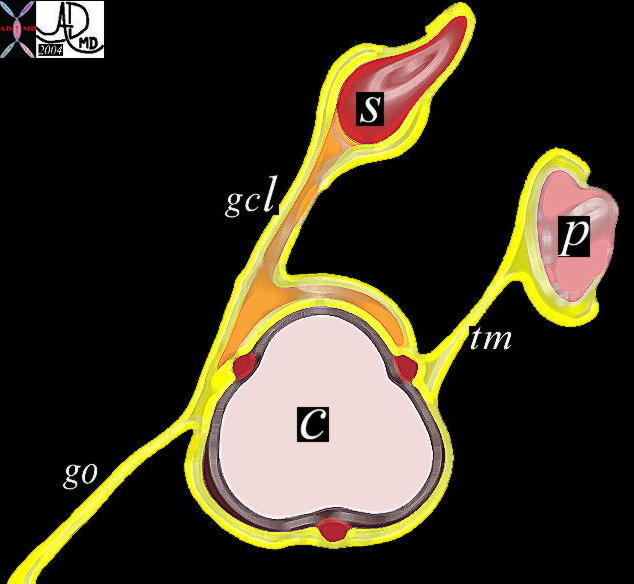
| In this diagram we demonstrate the relationship of the pancreas (p) with the posterior aspect of the colon (c) via the transverse mesocolon ™. The stomach (s) has a ligamentous relationship with the superior aspect of the colon via the gastrocolic ligament (gcl). Diseases of the pancreas can spread along the transverse mesocolon to the posterior border of the transverse colon, while diseases of the stomach may spread to the superior border of the transverse colon. The greater omentum (go) is the two layered apron of mesenteric fat that covers the organs of the abdomen anteriorly. 01443b05 Courtesy Ashley Davidoff MD |

Pancreas |
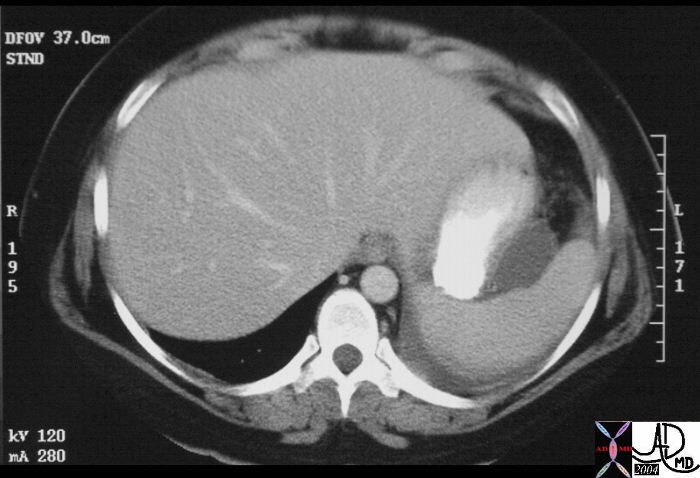
| This is the case of a 34 year old male with acute pancreatitis following and alcoholic binge. In this CT scan through the abdomen the inflammatory exudate and digestive enzymes have spread from the pancreas via the transverse mesocolon and to the serosa of the transverse colon. 39784 Courtesy Ashley Davidoff MD |

Pancreas |
| This is the case of a 34 year old male with acute pancreatitis following an alcoholic binge. In this CT scan through the abdomen there is thickening of the serosa of the transverse colon. The inflammatory exudate and digestive enzymes have spread from the pancreas via the transverse mesocolon and to the serosa of the transverse colon. Associated finding includes spread of the disease to the left paracolic gutter. 39785 Courtesy Ashley Davidoff MD |
Pancreas |
| This CT scan through the upper abdomen and lower chest shows a fluid accumulation in the splenic hilum and the left pleural space. The effusion is secondary to acute pancreatitis. 15734 Courtesy Ashley Davidoff MD |

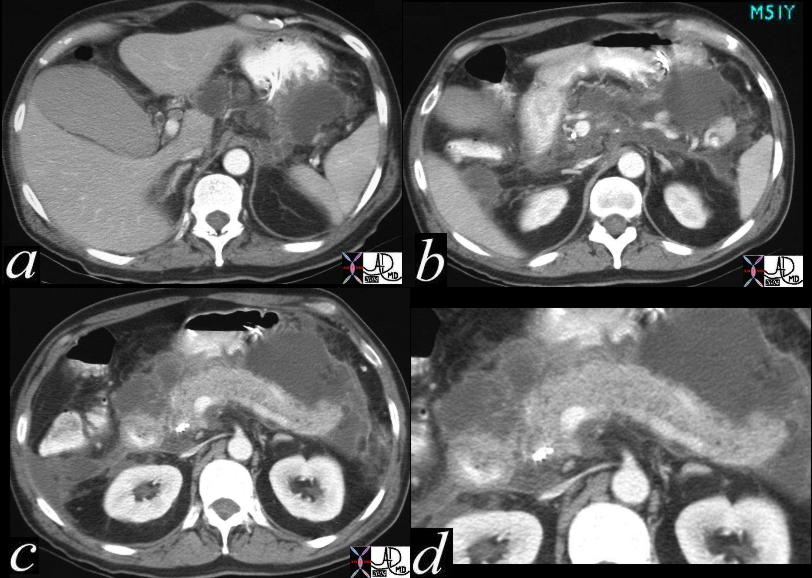
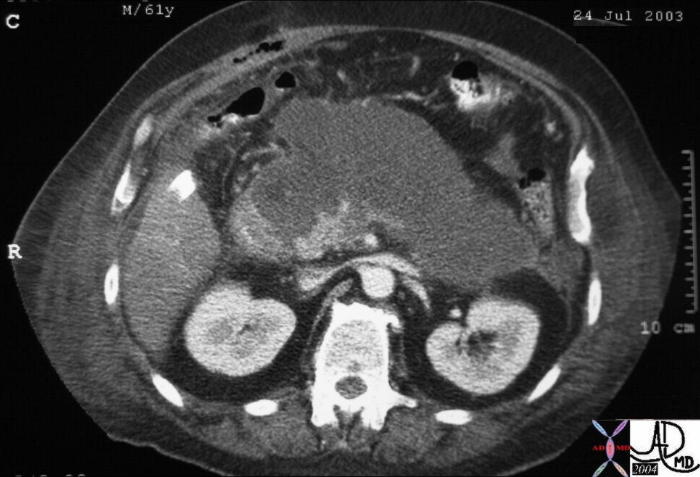
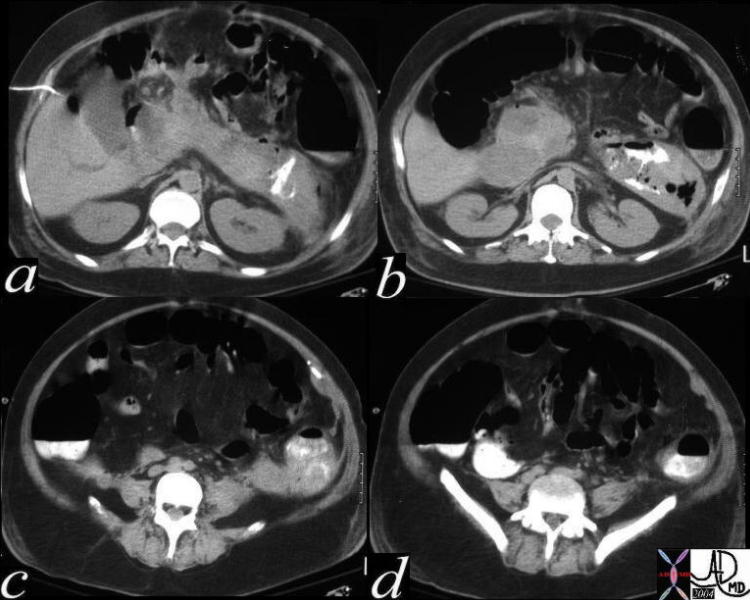
This is a CTscan of a 61 year old man who presents with abdominal pain, acute inferior myocardial infarction, with a background history of type II diabetes. The overall size of the pancreatic bed has increased mostly due to the peripancreatic effusion. The pancreas itself is only minimally enlarged and has a subtle increase in density suggesting hemorrhagic pancreatitis. It is sandwiched between the exudates anteriorly and posteriorly. Note the air in the lumen and the wall of the gallbladder consistent with emphysematous cholecystitis. Note also the changes in the left lateral conal fascia, and properitoneal fat suggesting transgression of fluid. Within both the hypodermis of both flanks there are soft tissue changes consistent with radiologic Gray-Turners sign. 31093 Courtesy Ashley Davidoff MD
Pancreas |
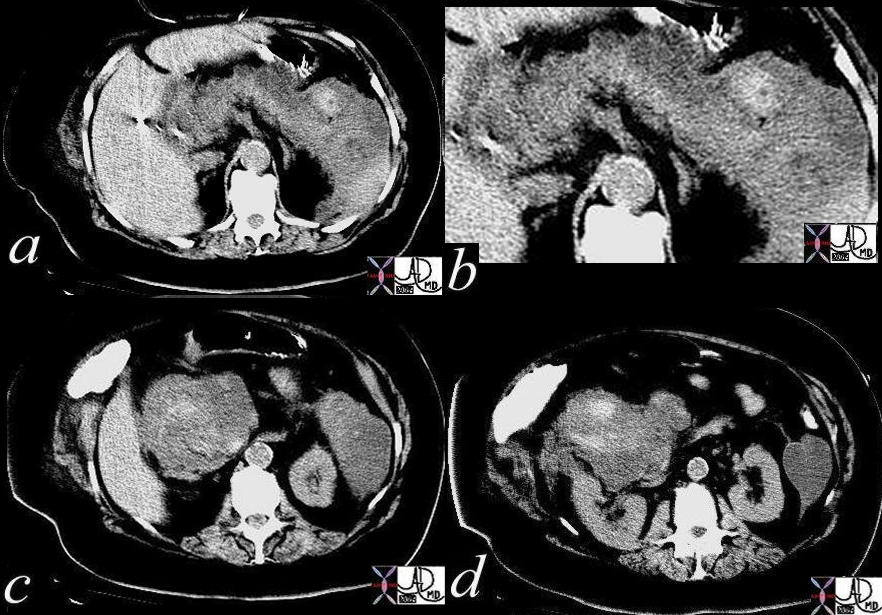
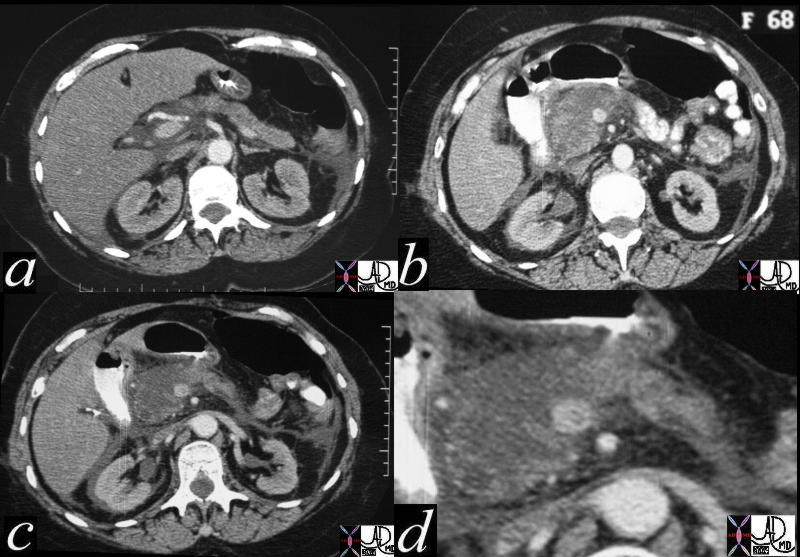
| This CT scan through the abdomen without iv contrast shows narrow windows of the accumulated fluid around the pancreas and in the paracolic gutters in a patient with acute pancreatitis. The findings are characterized by scattered areas of increased density in the pancreatic bed (a,b)as well as around the head of the pancreas. This is a case of hemorrhagic pancreatitis. 16851c02 Courtesy Ashley Davidoff MD |
Acute Pancreatitis – in the Transplanted Pancreas

Pancreas |
| This CTscan shows homogeneous enlargement of the pancreas in a 37 year female with long standing diabetes and renal failure. Surgical clips of a recent pancreatic transplant are noted on the anterior border of the transplant. This is a case of pancreatitis of the transplanted pancreas. 25329 Courtesy Ashley Davidoff MD |
Acute Pancreatitis – Traumatic
Pancreas |
| This series of CT scans through the pancreas show a vague hypodensity in the middle of the body of the pancreas (a, b) and a subtle change in texture of the tail of the pancreas (c,d). Subtle changes like those shown are often the findings in acute traumatic pancreatitis, since the time between injury and imaging is relatively short, and therefore structural changes are early in their evolution. A high level of suspicion should be maintained in patients with severe blunt abdominal trauma both by the ER physicians and radiologists since missing the diagnosis can be devastating. At surgery there was complete transaction of the pancreas. 40073c01 Courtesy Ashley Davidoff MD |
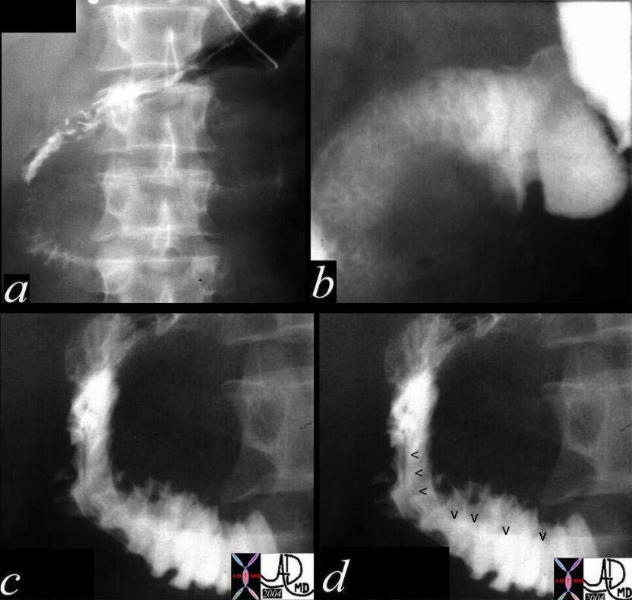
Pancreas |
| This upper GI study is of a young male who sustained blunt trauma to the abdomen and was complaining of abdominal pain. The images show the C-sweep of the duodenum which is widened, with extrinsic mass effect (arrowheads in d). The trauma to the abdomen was complicated by traumatic pancreatitis 18566c04 Courtesy Ashley Davidoff MD |
Acute Pancreatitis – Focal
Pancreas |
| This series of CT scans through the abdomen show a focal pancreatic phlegmon in the tail of the pancreas (a,b,c). The body and head of the pancreas were spared of inflammatory change. There is thickening of Gerota’s fascia seen in all the images, but exemplified in d. These findings are consistent with a focal pancreatitis of the tail. 40131c Courtesy Ashley Davidoff MD |
Acute Pancreatitis – Infection
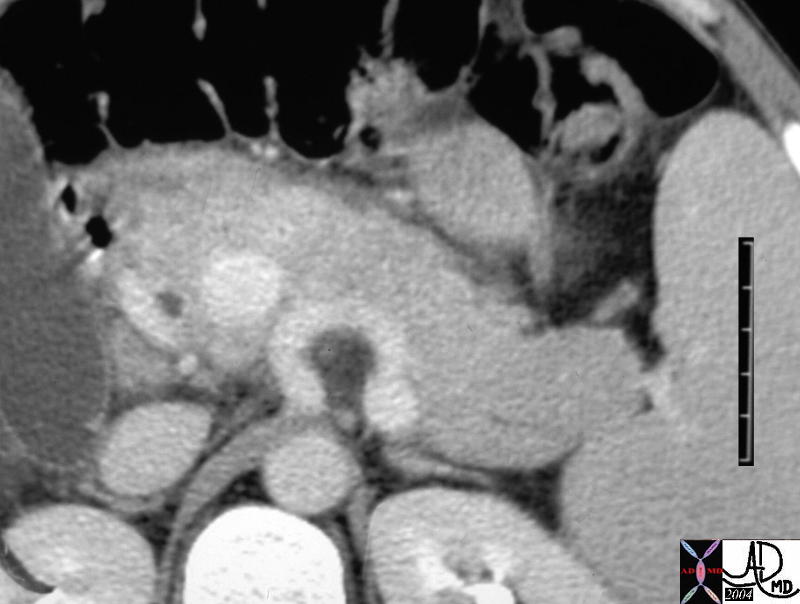
Pancreas |
| This coned down view of the CTscan of the pancreas of a young man with abdominal pain the tail of the pancreas is relatively large and the head relatively small consistent with the patients age. However on closer inspection there is a thin line of exudative fluid anterior to the pancreas in the anterior pararenal space. He was known to have both histoplasmosis and MAI and clinically his biochemistry was consistent with an infectious pancreatitis, most likely of MAI origin. 40092b01 Courtesy Ashley Davidoff MD |
|
Pancreas |
| Image c in this combination series of the CTscan of the pancreas of a young man with abdominal pain, shows prominence to the tail of the pancreas and a relatively large and the head relatively small consistent with the patients age. However on closer inspection there is a thin line of exudative fluid anterior to the pancreas in the anterior pararenal space. In a, there is fluid posterior to the pancreas, better seen in b, and there is fluid in Morrison’s pouch (d). He was known to have both histoplasmosis and MAI and clinically his biochemistry was consistent with an infectious pancreatitis, most likely of MAI origin. 40092b01 Courtesy Ashley Davidoff MD |
Subacute Pancreatitis – in the weeks following acute episode
The findings of an early organization of the collections with loss of the induration of the surrounding fat and the development of an enhancing rind, typify this phase of pancreatitis. The volume of the fluid accumulations increase when the pancreatic ductal system has been violated and is patent to the retroperitoneum.

Pancreas |
| This CT scan through the body of the pancreas shows a small pancreatic exudate around the uncinate process, body and tail of the pancreas.(phlegmon) The changes are well defined and there is little induration in the peripancreatic fat suggesting a subacute process. The findings are consistent with moderate subacute phlegmonous pancreatitis with the inflammatory process restricted to the anterior pararenal space. Associated findings include surgical clips in the gallbladder fossa. 39788 Courtesy Ashley Davidoff MD |
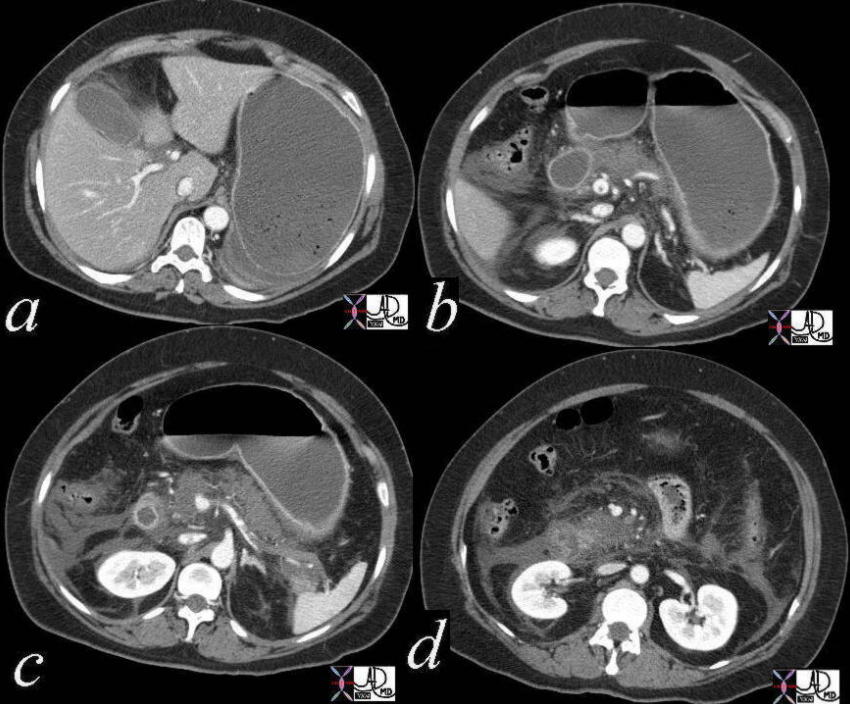
Pancreas |
| This combination CTscan shows the manifestations of severe acute alcoholic pancreatitis within the week or weeks following the acute episode. There is mild enlargement of the pancreas and significant phlegmonous changes characterized by a large peripancreatic exudate which has a enhancing rind around it suggesting the subacute nature of the disease. The exudate extends from the anterior pararenal space to the peritoneal cavity and into base of the mesentery. Associated findings include IVC thrombosis, with impingement and distortion of the greater curvature of the stomach. Severe steatosis of the liver with areas of sparing is also noted. 40277c Courtesy Ashley Davidoff MD |
Pancreas |
| This combination CTscan shows the manifestations of severe acute pancreatitis in a 51 year old male following the acute episode. The pancreas is slightly heterogeneous raising the possibility of piecemeal necrosis. The peripancreatic exudate of the phlegmonous pancreas has a rind of enhancing rim, suggesting a subacute nature. There is extension of the inflammatory process to both the paracolic gutters, and impingement and compression of the IVC and stomach. 26898c Courtesy Ashley Davidoff MD |
Pancreas |
| This combination CTscan shows the manifestations of acute pancreatitis. The enhancing rind on the fluid accumulation in b,c,and d, suggests the subacute nature. An early pseudocyst is seen in the head of the pancreas (a). The advancing inflammatory process has reached the anterior abdominal wall (d) and causes irritation and inflammation characterized by the enhancing peritoneum. 40139c02 Courtesy Ashley Davidoff MD |

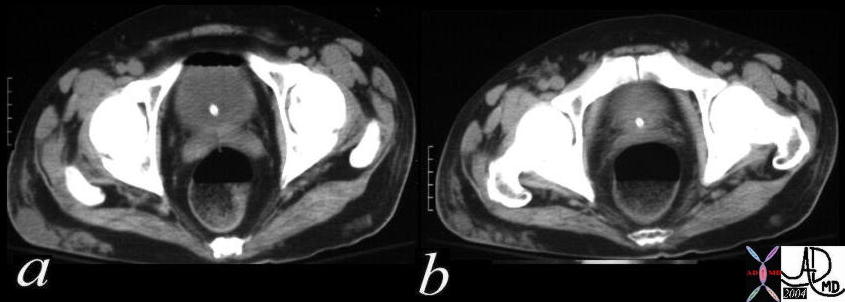
Pancreas |
| This CTscan of the pelvis is from a patient who was suffering from a severe episode of pancreatitis. In the region of the inguinal canal there is a fluid accumulation that is within the pelvic extension of the retroperitoneum. Associated findings include significant 3rd spacing of fluids. 41361 Courtesy Ashley Davidoff MD |
Pancreas |
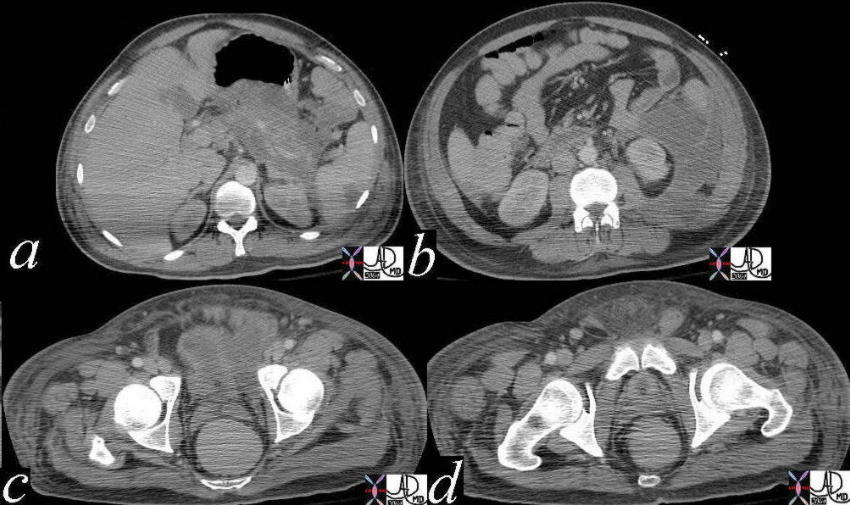
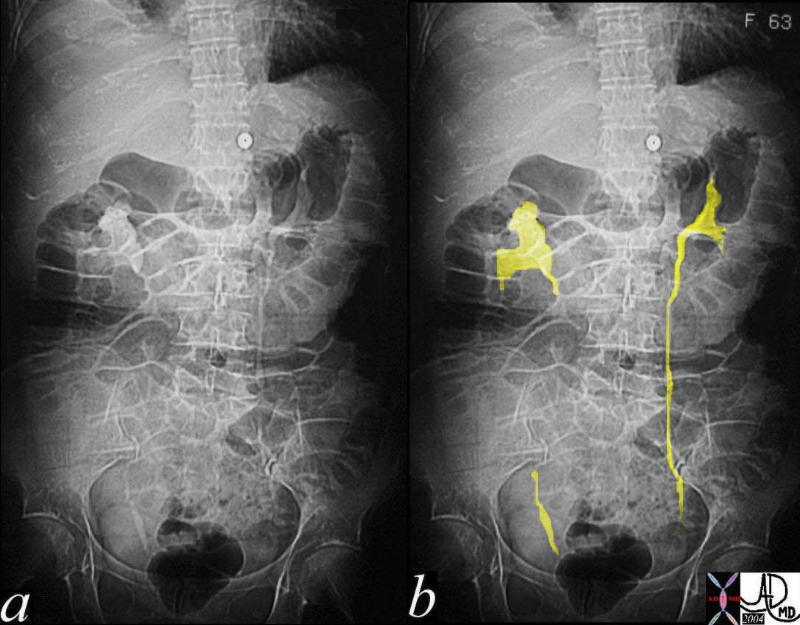
| This series of images are from a CTscan of a patient who was suffering from a severe episode of pancreatitis. The pancreas shows phlegmonous change and hypoperfusion suggestive of pancreatic ischemia or necrosis. The retroperitoneum is distended with advancing exudate dominating in the left anterior pararenal space. The fluid tracks all the way down to the pelvis (c) and then into the spermatic cord (d)In the region of the inguinal canal there is a fluid accumulation that is within the pelvic extension of the retroperitoneum.41362c01 Courtesy Ashley Davidoff MD |
Acute Pancreatitis – Pseudocyst Formation
Pancreas |
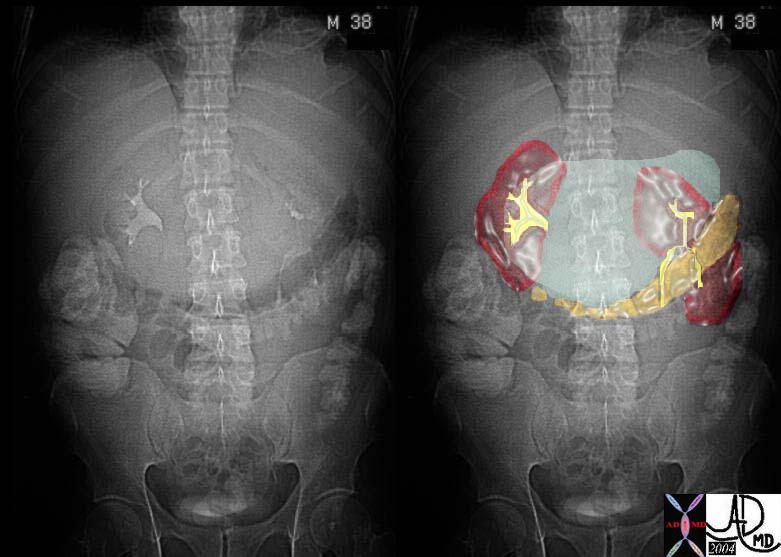
| This plain film of the abdomen shows the stomach displaced inferiorly by an enlarging pseudocyst in the lesser sac. In the second image the pseudocyst is outline in green, while he stomach is overlaid in orange. 40280c04 Courtesy Ashley Davidoff MD |
Pancreas |
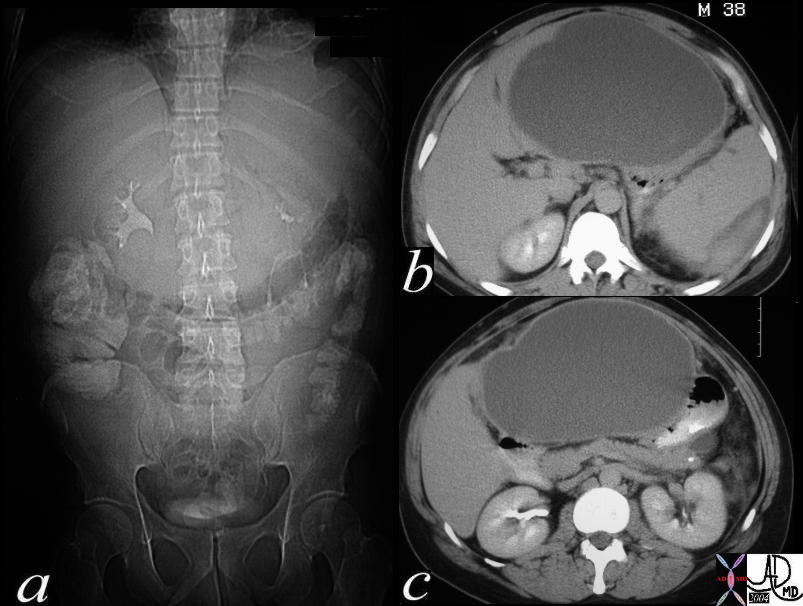
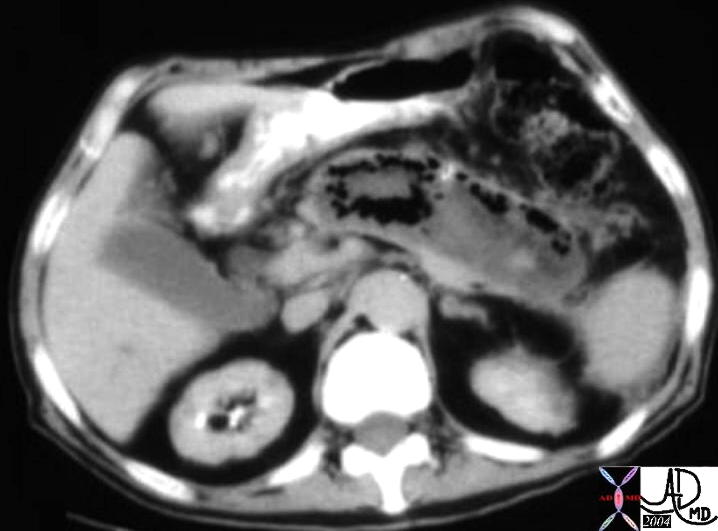
| This CTscan is of a 38 year old male with abdominal distension. The scout study shows inferior displacement of the transverse colon by a large epigastric mass. A large cystic structure impinging on the medial left lobe of the liver and the medial aspect of the stomach suggest a pseudocyst arising in the lesser sac from the pancreas and a diagnosis of a pancreatic pseudocyst secondary to acute alcoholic pancreatitis is most likely. The high density material around the spleen in b represents a subcapsular splenic hematoma. 40283c Courtesy Ashley Davidoff MD |
Acute Pancreatitis – Complications – Pseudoaneurym

Pancreas |
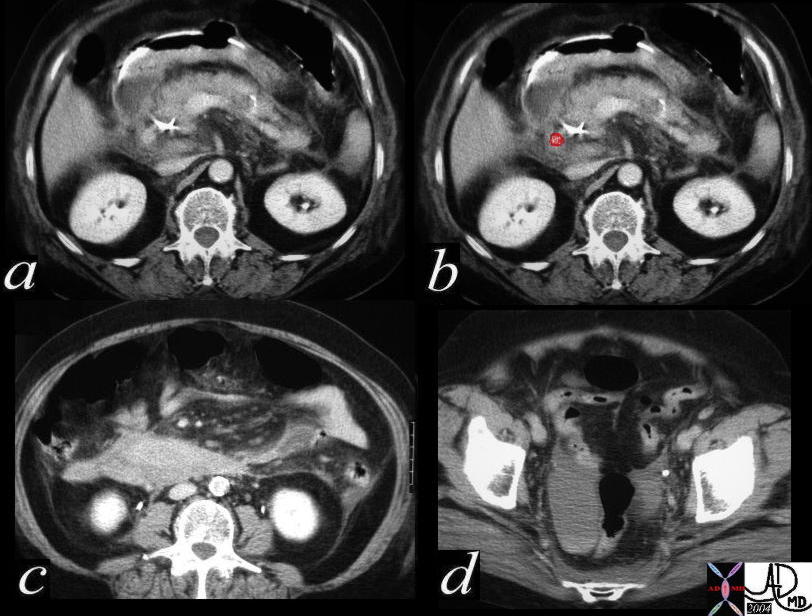
| This isthe CT scan through the abdomen of a patient who developed a drop in hematocrit in the days following an ERCP induced episode of acute pancreatitis. The findings include induration around the head of the pancreas, and thickening of Gerota’s fascia on the left. Associated findings include flattening of the IVC. Have we missed the most important life saving finding? Do you see a false aneurysm? What is the contrast accumulation posterior to the stent? This is a case of a pseudoaneurysm of a branch of the pancreaticoduodenal arcade. 40099 Courtesy Ashley Davidoff |
Pancreas |
| This is the CT scan through the abdomen of a patient who developed a drop in hematocrit in the days following an ERCP induced episode of acute pancreatitis. The findings include induration around the head of the pancreas, and thickening of Gerota’s fascia on the left, with a punctate accumulation of contrast posterior to a bright radioopacity (a). The pseudoaneurysm is overlaid in red (b). Hemorrhagic change is seen around the head in c, while a hematocrit level of acute blood is seen in d. The diagnosis is of a false aneurysm of a pancreaticoduodenal vessel. It was uncertain as to whether the pseudoaneurysm was induced by the pancreatitis or by the sphincterotomy. 40099c02 Courtesy Ashley Davidoff MD |
Pancreas |
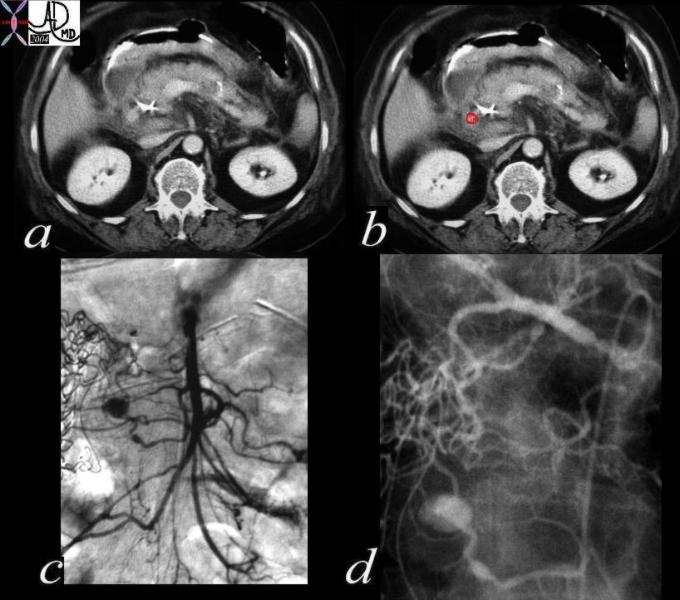
| This is a combination of CT scan and an angiogram through the abdomen of a patient who developed a drop in hematocrit in the days following an ERCP induced episode of acute pancreatitis. The findings on the CT scan include induration around the head of the pancreas, and thickening of Gerota’s fascia on the left, with a punctate accumulation of contrast posterior to a bright radioopacity (a). The pseudoaneurysm is overlaid in red (b). The angiogram in c shows the pseudoaneurysm off the inferior pancreaticoduodenal branch from an SMA injection, while the aneurysm is demonstrated in d after an injection into the hepatic artery. It was uncertain as to whether the pseudoaneurysm was induced by the pancreatitis or by the sphincterotomy. 40099c04 Courtesy Ashley Davidoff MD |
Pancreas |
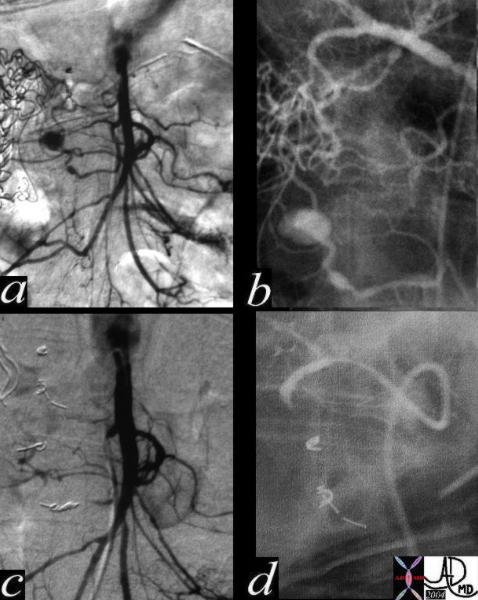
| This is a combination of angiograms performed before (a,b) and after (c and d) in a patient who developed pancreatitis and a drop in hematocrit following ERCP and a sphincterotomy. In the SMA injection (a) a focal well defined accumulation of contrast represents a pseudoaneurysm of a branch of the inferior pancreaticoduodenal artery. The pseudoaneurysm is also demonstrated in a hepatic arterial injection that fills the pancreatic arcade via the gastroduodenal artery. After embolization the aneurysm has been occluded. (c,d) 40099c05 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Necrosis

Pancreas |
| This CT scan through the abdomen shows heterogeneous enhancement of the pancreatic head following an acute episode of the pancreas. Associated findings include bilateral thickening of Gerota’s fascia, perirenal induration on the right and thickening of the peritoneum of the left. 19888 Courtesy Ashley Davidoff MD |
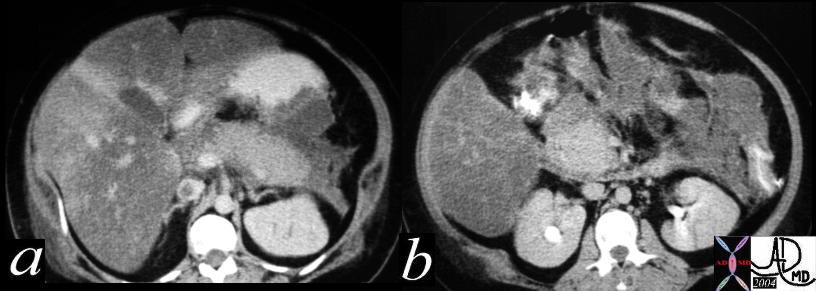
Pancreas |
| This combination CT scan through the abdomen shows heterogeneous enhancement of the pancreatic head and tail (a,b) following an acute episode of the pancreas. Associated findings include bilateral thickening of Gerota’s fascia, perirenal induration on the right and thickening of the peritoneum of the left. Closer inspection of the head (d) shows hypoperfusion, a finding consistent with pancreatic necrosis. 19892c Courtesy Ashley Davidoff MD |
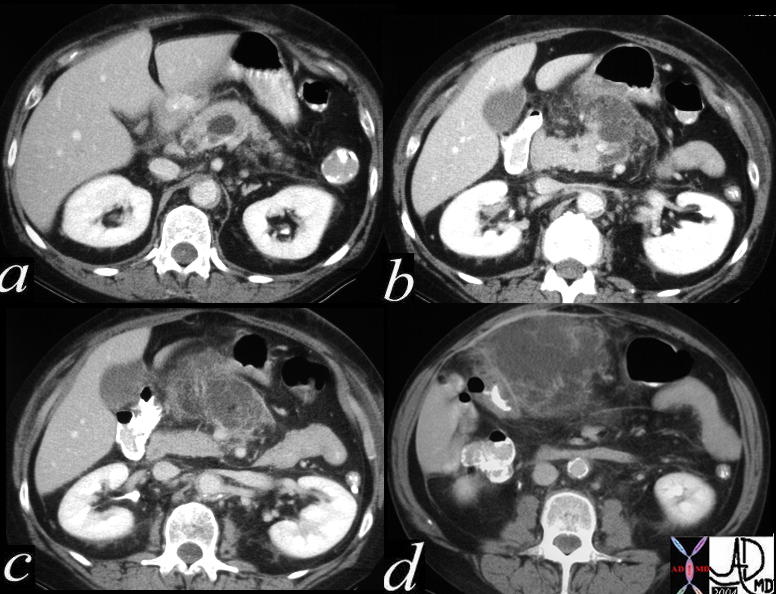
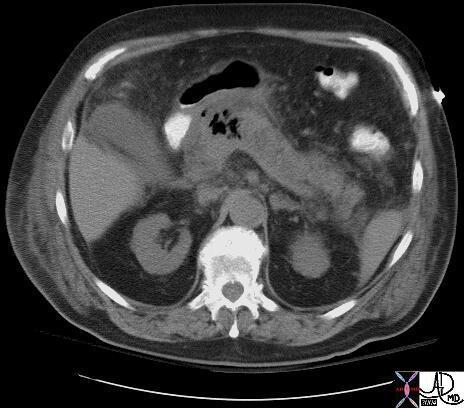
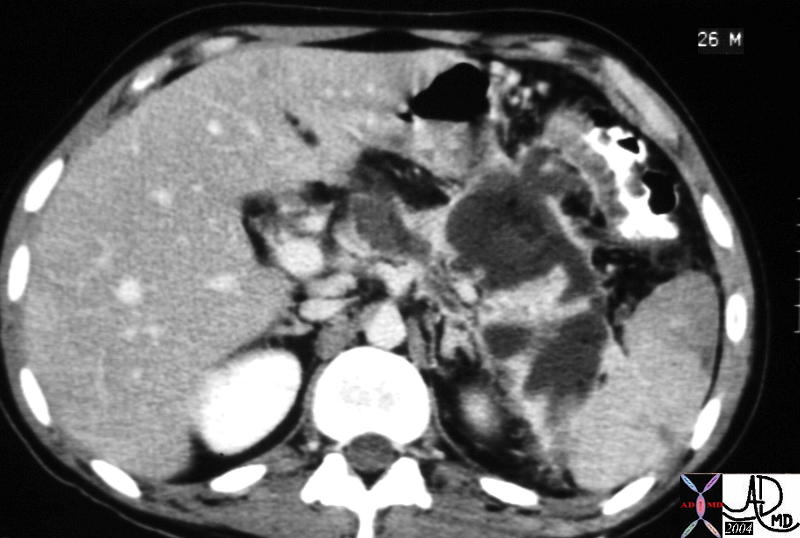
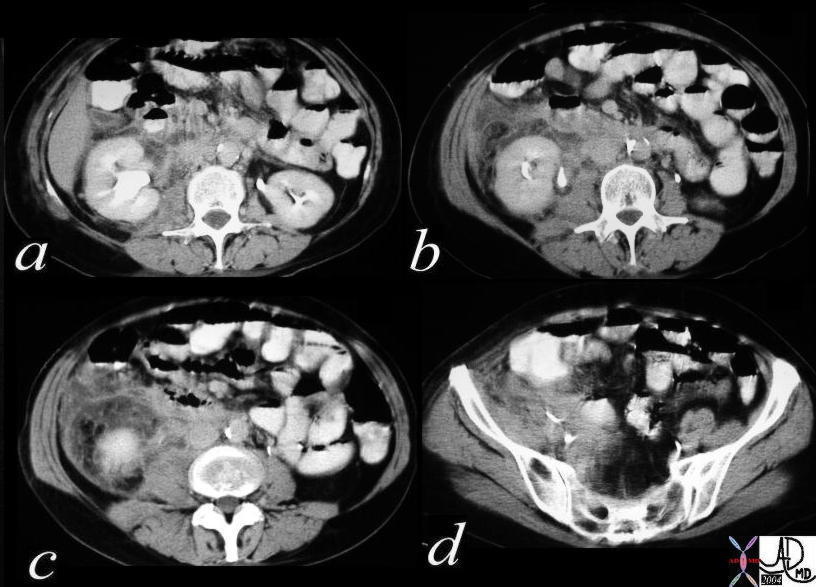
The CT scan of the abdomen of a 61 year old male shows a large cystic type lesion in the lesser sac, conforming to the shape of the pancreas. Note also the piecemeal appearance of the remaining viable pancreas in the region of the uncinate process. There was little other viable pancreas identified and a diagnosis of pancreatic necrosis was made. Associated findings include extension of the inflammatory process to the left paracolic gutter and through to the soft tissues of the flanks, as well as postoperative air in the right rectus abdominis muscle. 31188b01 Courtesy Ashley Davidoff MD
Pancreas |
| This CT scan through the abdomen shows air in the head of the pancreas associated with induration around the pancreas, gallbladder and hypodermis of the skin. The findings are consistent with pancreatic necrosis. 19610 Courtesy Ashley Davidoff MD |
Pancreas |
| This is a CT of an elderly man who had severe pancreatitis. Within the pancreatic bed there is a structure that conforms to the shape of the pancreas. It is enlarged and consists mostly of air, fluid, and high density hemorrhagic components. The findings are consistent with a gangrenous pancreatic abscess. The surgeon noted that the pancreas looked and smelled like a “dead fish…. that had been dead for quite a long time.” 04959 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Thrombosis
Pancreas |
| This is a CTscan through the abdomen of a patient who had recovered from a severe acute episode of pancreatitis. IVC thrombus is seen (a), while in b a pseudocyst in the head of the pancreas, is shown to compress the IVC. 40168c01 Courtesy Ashley Davidoff MD |
Pancreas |
| This combination of CTscan and IVC venogram is from the records of a patient who had recovered from a severe acute episode of pancreatitis. IVC thrombus is seen (a), and is confirmed as a filling defect in the cavagram (c,d) A pseudocyst in the head of the pancreas is shown to compress the IVC. (b) 40171c02 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Local Invasion of the Spleen
It is not uncommon for the process to extend to the left upper quadrant and affect the splenic vein splenic flexure and sometimes even the splenic artery.
Pancreas |
| This 26 year old patient with acute alcoholic pancreatitis shows a large accumulation of complex fluid in the LUQ with invasion into the hilum of the spleen. There are multicentric wedge shaped defects in the spleen and thickening of the colon. The presumed infarctions in the spleen are unusual, and arterial encasement is the most likely cause. 40249 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Local Invasion of the Stomach
Pancreas |
| This CTscan of the abdomen is from the records of a patient who presented with vomiting following a recent episode of pancreatitis. The findings show a fluid filled stomach with sediment of more solid contents in the dependant parts of the fundus. (a,b) There is narrowing and then obstruction of the gastric outlet (c,d) with footprints of pancreatitis in the anterior pararenal space (d). This case is an example of gastric outlet obstruction following acute pancreatitis. 41531c01 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Local Invasion of the Colon
Pancreas |
| This CT scan through the abdomen following an abscessogram of a drained pseudocyst that had originally complicated a hemorrhagic pancreatitis. The study shows contrast in the splenic flexure. The pseudocyst had formed a fistulous tract to the colon 40152c02 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Local Invasion of the Ureter
Pancreas |
| This 63 year old female presented with acute abdominal pain. The scout film following the CTscan of the abdomen shows right sided hydronephrosis with a suggestion of an obstruction at the level of the UPJ. 40292bc01 Courtesy Ashley Davidoff MD |
Pancreas |
| This abdominal CT scan shows extensive inflammatory change surrounding the right kidney in the anterior pararenal and perirenal spaces extending into the pelvis. There is hydronephrosis of the left kidney. These findings are consistent with hydronephrosis of the left kidney secondary to the pancreatitis. 40299c01 Courtesy Ashley Davidoff MD |
Acute Pancreatitis
Complications – Systemic Effects
|
Pancreas |
| This CT scan of the pelvis shows soft tissue changes in the hypodermis of the right buttock, and a small soft tissue density in the left buttock. This patient had experienced a remote episode of pancreatitis complicated by IVC thrombosis and infarcts in the tibia. The suggested diagnosis is fat necrosis or saponification of subcutaneous fat caused by circulating lipases released during the acute episode. 40171c01 Courtesy Ashley Davidoff MD |
Pancreas |
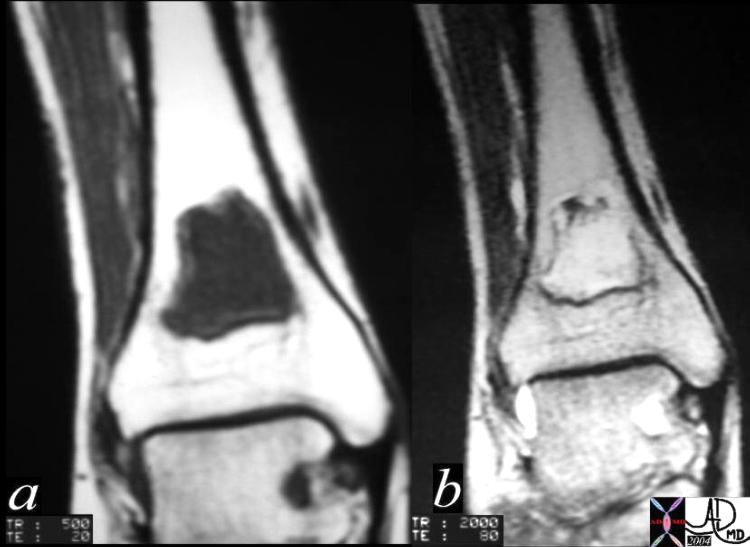
| This MRI of the tibia shows an infarct in the distal tibia. This patient had experienced a remote episode of pancreatitis complicated by IVC thrombosis and fat necrosis of the buttock fat. The suggested diagnosis is marrow necrosis or saponification caused by circulating lipases released during the acute episode.
40188c02 Courtesy Ashley Davidoff MD |