| The Common Vein copyright 2008
Introduction
In this section we expand on the features that describe the organ and are used to identify and ditinguish between normal morphology an abnormal morphology. We always evaluate the organ in terms of its size, shape, position and characteristics.
Size of the Pancreas
In this section we deal with the various criteria that are used to assess the size of the pancreas. As one reviews the pancreas among the young and the old, males and females and among different individuals, it is no surprise to find that each pancreas has a unique face and that pancreatic size has a wide variation. Measurements should therefore only be used as a rough guide in the evaluation of size, and other factors such as shape, character and perfusion characteristics are key in the overall morphological evaluation.
Guidelines
There are absolute measurements that one can use if subjectivity of the size assessment fails. These measurements are outlined below.
A-P dimensions (approximations)
head about 2.5 cm -3.5cms.
neck about .8cms-1.5cms
body about 1.5cm – 2.5cm
tail about 1.5 cm-3.5cms.
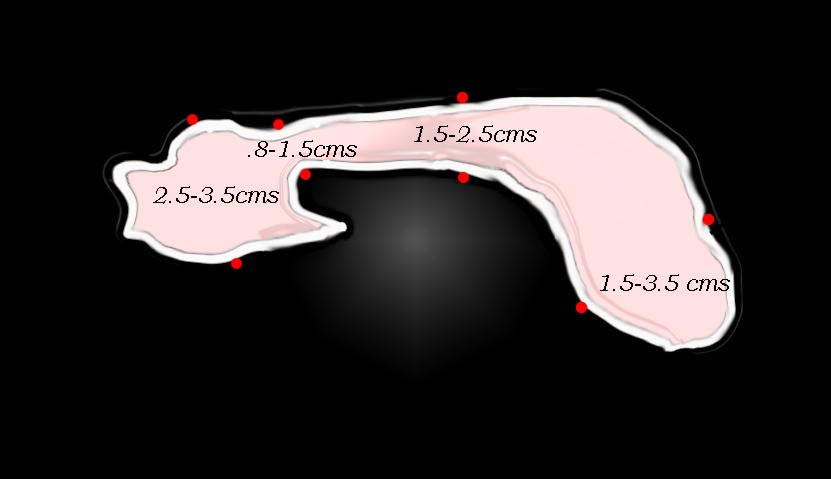 Size of Head Neck Body and Tail Size of Head Neck Body and Tail |
| The measurements vary significantly betwen individuals, but usual measurements aredefined in the above drawing. 41394size002b01 Courtesy Ashley Davidoff MD |
Weight: 60 to 100 gm
Length 12-15 cm in length
In young patients, the body or the tail may be larger than the head, whereas in people over 40 the head assumes larger proportions than the body and tail. When the pancreas is young, the surface of the pancreas is relatively smooth. As it ages the earliest signs of volume loss is development of a nodular shape of the surface. Thus the shape deformity reflects an involutional process and assessment of the shape gives insight into the size and approximate age of the gland.
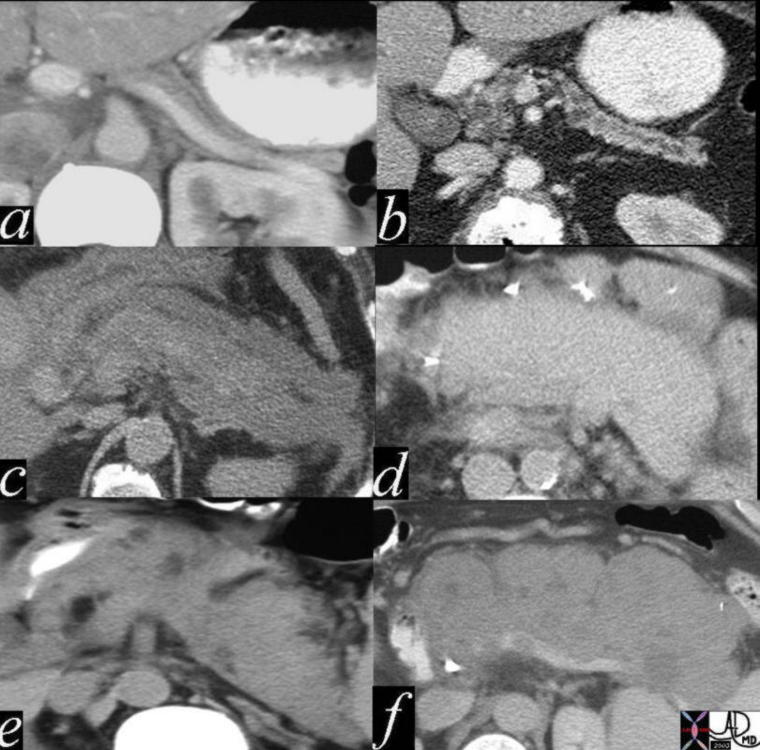
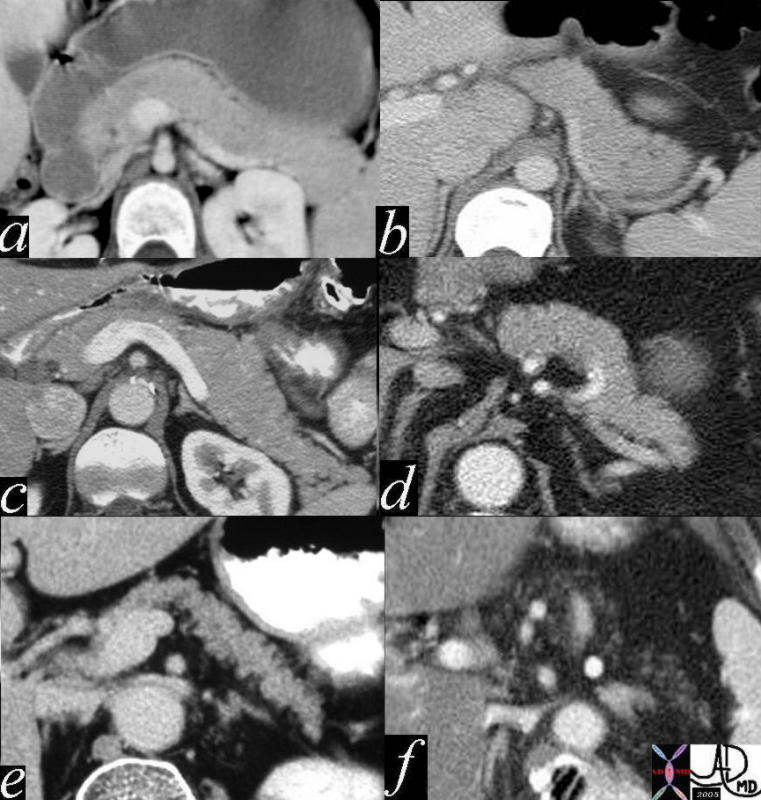 The size of the tail varies considerably between individuals, but in general it is relatively large in youth (a,b) starts to thin in middle age (c,d) and atrophies in the elderly (e,f) a= 12 year old female b= 30 year old female c= 30 year old male d= 40 year old male e= 70 year old female f = 80 year old female41394size02 Courtesy Ashley Davidoff MD The size of the tail varies considerably between individuals, but in general it is relatively large in youth (a,b) starts to thin in middle age (c,d) and atrophies in the elderly (e,f) a= 12 year old female b= 30 year old female c= 30 year old male d= 40 year old male e= 70 year old female f = 80 year old female41394size02 Courtesy Ashley Davidoff MD
This involutional change with age is very common and most of the time has no clinical significance. In fact sometimes the pancreas is almost completely replaced by fat, and it still functions normally. While the overall volume of the pancreatic tissue may be normal there is volume loss of glandular and interstitial tissue with secondary fat infiltration. Thus the character of the gland with the presence of fat gives insight into the size of the glandular mass. For the pancreas to lose exocrine function, more than 90% of exocrine pancreatic tissue needs to be lost . Clinical presentation in that instance would include failure to thrive, steatorrhea, fat intolerance, abdominal pain, bloating, and flatulence. With aging there is an increased incidence of type II diabetes. This is probably not only as a result of critical loss of beta cells from the islets, but also other factors that relate to decreased efficacy of the insulin.
There are observed experimental changes in the size of the pancreas during differing physiological states. During digestive process, the gland is most active, and swells as it secretes hormones and enzymes. These changes are not visible on coventional imaging.
Sometimes the pancreatic duct size gives a clue to pancreatic volume. Chronic obstruction of the duct will lead to atrophy of the gland. This may be due to a stone in the duct, or a neoplasm in the neck or head. A relative discrepancy in the size of the tail and the size of the head in the presence of a dilated pancreatic duct raises the distinct probabability of an upstream panctreatic carcinoma or obstructing benign mass or stone.
Neck of the Pancreas
The neck of the pancreas usually merges imperceptibly with the body and head. In general as we view the pancreas in the transverse plain, the neck is marked by point where the globular head thins out into the more rectangular shaped neck. Like the neck of most structures its overall size is less than the head and the body which it connects. It can however be short and fat or long and thin. Its stated range of A-P dimension is .8-2.5cms while its lenth is in the 1.5-2cms range
Anteriorly its rightward border is marked by the gastroduodenal artery and the groove for this vessel sometimes forms a distinct notch in the neck in which case the border is delineated by a focal constriction. The left margin anteriorly is marked by the tuber omentale, a focal prominence, which abuts the posterior surface of the lesser omentum.
CAN THE PANCREAS REGENERATE, HYPERTROPHY OR UNDERGO HYPERPLASIA?
The animal experiments that are available would suggest that there is a limited ability of both the exocrine portion and the beta cells to grow – both by hypertrophy and by hyperplasia(Oates)
B cell growth
The beta-cell mass in the adult pancreas possesses the ability to undergo limited regeneration following injury. (Dickson, Hardikar)
Volume loss in pancreatitis
(Madro)
Diffuse thinning of the gland is more common than diffuse enlargement. Overall volume loss of the gland is usually caused by aging, chronic pancreatitis, or by an obstructed pancreatic duct. Diffuse enlargement of the gland may be caused by acute pancreatitis, lymphoma and and metastasis to the gland. Less common diseases such as von Hippel Lindau, hemangioma, Merckl cell tumor, sarcomas, and VIPOMAS are usually associated with unusual contour deformities and heterogeneous morphology of the gland. There is an unusual disease called pseudohypertrophy
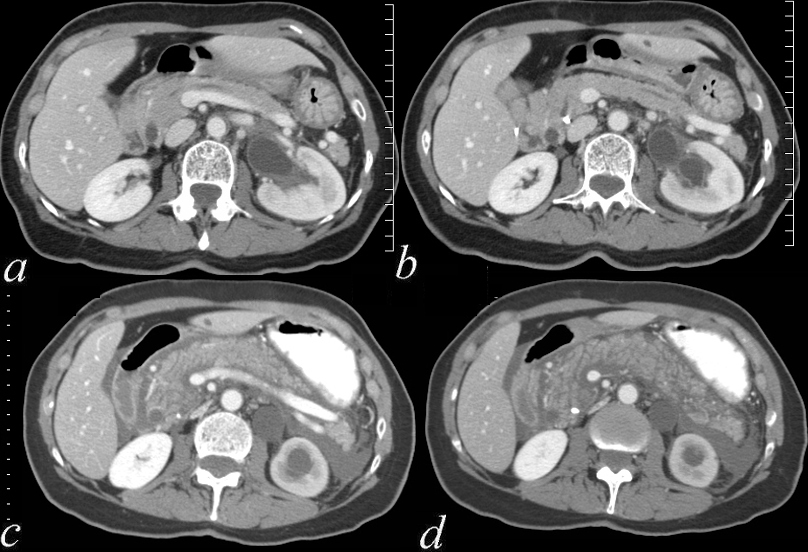
This series of six images show a normal pancreas from superior to inferior. The tail being the most superior first comes into view, and then the body, head and finally the uncinate process. The duct is seen as a faint lucency in c. Courtesy Ashley Davidoff MD 38031c01 code pancreas normal code pancreas normal anatomy
41394size02 Courtesy Ashley Davidoff MD code pancreas size normal anatomy a= 12 year old female b= 30 year old female c= 30 year old male d= 40 year old male e= 70 year old female f = 80 year old female
41394size03 Courtesy Ashley Davidoff MD code pancreas size normal anatomy imaging radiology USscan
Size of the Pancreatic Duct
The average maximum diameter of the main pancreatic duct (autopsy series), was 2.9 mm (<50yrs) and 3.5 mm (>50years).
On ERCP the duct is 3 to 4 mm in the head, 2 to 3 mm in the body, and 1 to 2 mm in the tail.
The upper limits of a normal duct diameter on CT is considered to be 2 to 3 mm in the body and tail, and up to 5 mm in the head.
The length of the pancreatic duct is variable; however, mean length is approximately 205 mm, with a range of 107 to 270 mm.
Two areas of narrowing may be seen normally at the orifice of the duct and at the junction of the dorsal and ventral fusion site in the head. When the narrowing is a normal variant there will be no upstream dilitation and the postdrainage study will show clearing of the contrast from the system
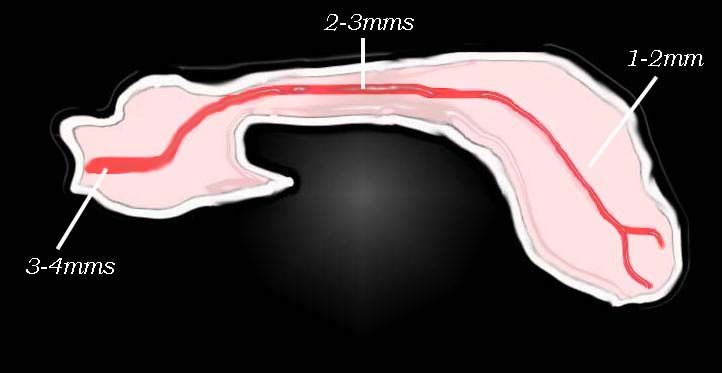 Size of Duct Size of Duct |
| The size of the duct varies according to the type of study conducted, bu ingeneral the normal and usual sizes are described above. 41394size002b02L Courtesy Ashley Davidoff MD code pancreas pancreatic duct normal drawing anatomy normal size |
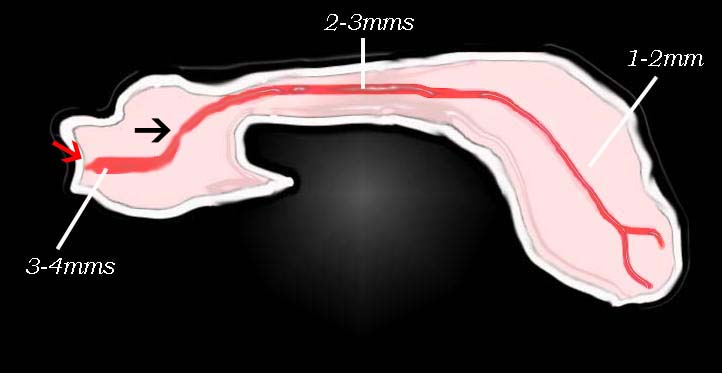 Normal Narrowings Normal Narrowings |
| There are two normal narrowings that may be seen. The first (red arrow) is the normal constriction of the pancreatic duct sphincter. The second is sometimes seen in the neck at the junction of the dorsal and ventral components of the duct (black arrow). 41394size002b04L Courtesy Ashley Davidoff MD |
Size of the The Ampulla
varies in width from 1.5mms to 4.5mms and its lenth varies from 1-14mms
Size of the Islets Of Langerhans
Suprisingly the islets of Langerhans represent only 1-2% of the volume of the pancreas and this represents about 1 million islets. The islets weigh in total g between 1.0 and 1.5 g, or 1/100th of the total weight of the pancreas. They are most numerous in the tail.
Exocrine Portion
The glandular constituents by weight are 80% exocrine tissue, 18% ductal system and intersttium, and 2% endocrine tissue.
Application To Disease:
A small pancreas is much more common than a large pancreas in diseases. However since the size of the pancreas is so variable and the pancreas decreases in size with age even a “small” pancreas could be normal. If however, the duct is enlarged in the presence of the small pancreas, then an upstream pathological process should be sought.
Diffuse enlargement of the pancreas is an uncommon finding and is usually restricted to metastatic disease, or lymphoma.
Application To Imaging:
Unlike most organs that are inflammed the relative degree of swelling and enlargement of the pancreas in severe pancreatitis is minimal. This is probably because the pancreas has very little in the way of a capsule and most edematous changes leak out from the pancreas causing a more dominant peripancreatic accumulation of fluid.
 The series of CT scans through a variety of entities is shown. In a there is exterme atrophy of the gland, but with a normal duct. This finding may be normal. In b there is atrophy associated with a dilated duct. This finding is usually abnormal and is usually caused by pancreatitis or carcinoma. Diffuse enlargement of the pancreas is uncommon and in the above cases is caused by hemorrhagic pancreatitis (c), pancrreatitis in a transplanted kidney (d), von Hippel Lindau syndrome (e) and metastatic Merkel cell tumor (f) Enlargement 41394csize04 Courtesy Ashley Davidoff MD code pancreas size abnormal small enlarged anatomy imaging radiology CTscan The series of CT scans through a variety of entities is shown. In a there is exterme atrophy of the gland, but with a normal duct. This finding may be normal. In b there is atrophy associated with a dilated duct. This finding is usually abnormal and is usually caused by pancreatitis or carcinoma. Diffuse enlargement of the pancreas is uncommon and in the above cases is caused by hemorrhagic pancreatitis (c), pancrreatitis in a transplanted kidney (d), von Hippel Lindau syndrome (e) and metastatic Merkel cell tumor (f) Enlargement 41394csize04 Courtesy Ashley Davidoff MD code pancreas size abnormal small enlarged anatomy imaging radiology CTscan
Atrophy of the upstream pancreas secondary to ductal dilatation is more common and more easily recognised. Space occupying diseases, such as primary or metatstatic carcinoma of the pancreas lymphoma and von Hippel Lindau result in an enlarged pancreas. There is an unusual and rare disease called lipomatous pseudohypertrophy of the pancreas that results in both diffuse enlargement and diffuse fatty infiltration that once seen will never be forgotten.
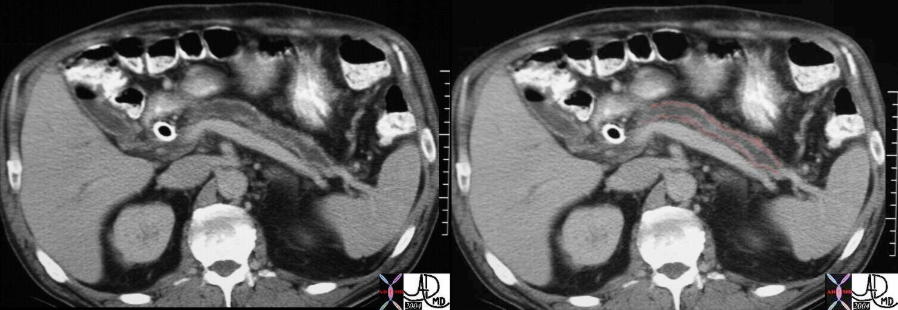 The CT scan through the abdomen in this case shows a dilated duct, atrophied pancreas (pink), and a stent in the CBD. In this case pancreatic carcinoma caused obstruction of the duct with secondary atrophy of the gland.. 16312c Courtesy Ashley Davidoff MD The CT scan through the abdomen in this case shows a dilated duct, atrophied pancreas (pink), and a stent in the CBD. In this case pancreatic carcinoma caused obstruction of the duct with secondary atrophy of the gland.. 16312c Courtesy Ashley Davidoff MD
 Before and After Acute Pancreatitis Before and After Acute Pancreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid |
| 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02 |
 This diffuse enlargement of the gland on the CT scan through the abdomen is secondary to enlarged pancreatic lymph nodes in this patient with lymphoma. Note the prominent retrocrural nodes and the ascites. With this degree of retrocrural lymphadenopathy that is sufficient to cause deformity of the aorta, chylous ascites must be considered. 29945 Courtesy Ashley Davidoff MD This diffuse enlargement of the gland on the CT scan through the abdomen is secondary to enlarged pancreatic lymph nodes in this patient with lymphoma. Note the prominent retrocrural nodes and the ascites. With this degree of retrocrural lymphadenopathy that is sufficient to cause deformity of the aorta, chylous ascites must be considered. 29945 Courtesy Ashley Davidoff MD
 This diffuse enlargement of the gland on the CT scan through the abdomen is secondary to enlarged pancreatic lymph nodes in this patient with metatstattic Merkel cell tumor. Note the enlarged venous collateral anterior to the pancreas, the focal filling defect in the splenic vein both suggesting the occlusion or high grade stenosis of the splenic vein. 22322 Courtesy Ashley Davidoff MD This diffuse enlargement of the gland on the CT scan through the abdomen is secondary to enlarged pancreatic lymph nodes in this patient with metatstattic Merkel cell tumor. Note the enlarged venous collateral anterior to the pancreas, the focal filling defect in the splenic vein both suggesting the occlusion or high grade stenosis of the splenic vein. 22322 Courtesy Ashley Davidoff MD
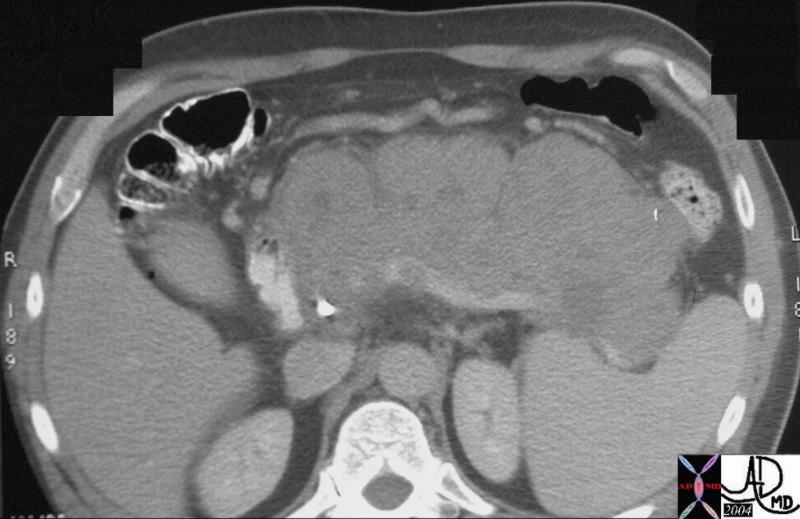
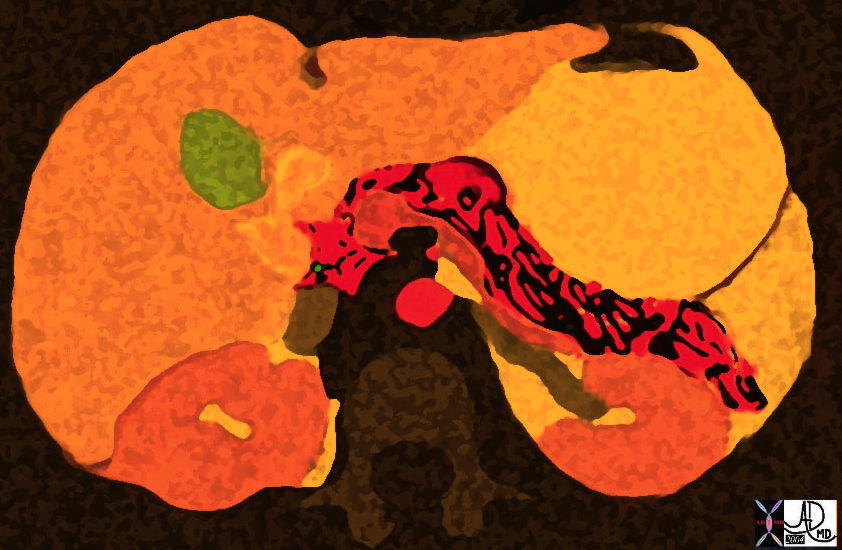 Pancreas in the Fall just before Halloween 38025b12 Courtesy Ashley Davidoff MD Pancreas in the Fall just before Halloween 38025b12 Courtesy Ashley Davidoff MD
The retroperitoneum is divided into three major compartments – the anterior pararenal space, the perirenal space and the posterior pararenal space. The pancreas lies in the anterior pararenal space, and shares this space with the transverse duodenum, and great vessels. The latter have been given a subcompartment by some authors, called the central retroperitoneum, since the great vessels seem to be protected from anterior pararenal space disease.
Long Axis:
Its axis is therefore dominantly but not strictly transverse.
The pancreas extends from the duodenal loop to the splenic hilum diagonally across the body at about the L1 -L2 level It can be divided anatomically into a head, neck, body, and tail. 4 The neck lies anterior to the superior mesenteric vein and proximal portion of the main portal vein formed by the confluence of the superior mesenteric and splenic veins. The head of the pancreas lies lateral to the neck, nestled in the C-loop of the duodenum. In this area it lies anterior to the inferior vena cava and right crus of the diaphragm. The inferomedial portion of the head is called the uncinate process, which varies greatly in size. It lies posterior to the superior mesenteric vein and, in about 5c% of patients, it lies posterior to the proximal superior mesenteric artery. The body of the pancreas lies anterior to the abdominal aorta below the origin of the celiac axis and anterior to the origin of the superior mesenteric artery. The tail is anterior to the left crus of the diaphragm, the left adrenal gland, and the left kidney, from which it is separated by the anterior portion of Gerota’s fascia
|