|
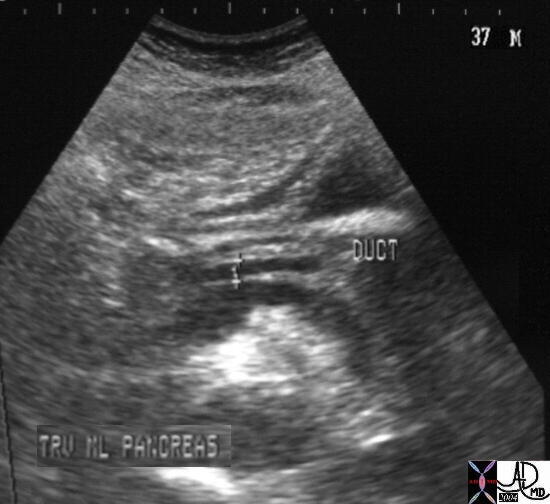 This US scan is from a 37 year old male showing a duct that appears to be mildly enlarged. It measured 4mms which is abnormal, but the error of measurement using electronic calipers is notoriously inaccurate. The duct however certainly looks dilated. Many times enlargement is a subjective interpretation. Sometimes a fatty meal is given to determine whether the dilatation will change with the fatty meal as the pancreas responds with increased secretion. If the duct measurement increases with the fatty meal an obstruction is suspected. 28948 Courtesy Ashley Davidoff MD This US scan is from a 37 year old male showing a duct that appears to be mildly enlarged. It measured 4mms which is abnormal, but the error of measurement using electronic calipers is notoriously inaccurate. The duct however certainly looks dilated. Many times enlargement is a subjective interpretation. Sometimes a fatty meal is given to determine whether the dilatation will change with the fatty meal as the pancreas responds with increased secretion. If the duct measurement increases with the fatty meal an obstruction is suspected. 28948 Courtesy Ashley Davidoff MD
 This 58 year old female presents with recurrent acute episodes of severe abdominal pain. This CTscan shows heavy calcification of the body and tail with a segment in the middle of a dilated pancreatic duct. The findings are consistent with chronic alcoholic pancreatitis. 41241 Courtesy Ashley Davidoff MD This 58 year old female presents with recurrent acute episodes of severe abdominal pain. This CTscan shows heavy calcification of the body and tail with a segment in the middle of a dilated pancreatic duct. The findings are consistent with chronic alcoholic pancreatitis. 41241 Courtesy Ashley Davidoff MD
 This CT scan through the pancreas shows a hypodense mass in the pancreatic head, associated with a central dystrophic calcification and a dilated pancreatic duct. These findings are consistent with a cystadenoma, and a malignant transformation of a mucinous neoplasm has to be considered in view of the dilated duct. The calcifications in the spleen are granulomatous in origin. 19394c01 Courtesy Ashley Davidoff MD This CT scan through the pancreas shows a hypodense mass in the pancreatic head, associated with a central dystrophic calcification and a dilated pancreatic duct. These findings are consistent with a cystadenoma, and a malignant transformation of a mucinous neoplasm has to be considered in view of the dilated duct. The calcifications in the spleen are granulomatous in origin. 19394c01 Courtesy Ashley Davidoff MD
 This CT scan through the pancreas shows a mass in the neck associated with pancreatic duct dilatation and secondary atrophy in the pancreatic tail. These findings are consistent with a diagnosis of a primary carcinoma of the pancreas. Based on the desmoplastic nature of the process the tumor is most likely a scirrhous adenocarcinoma. 30101a05 Courtesy Ashley Davidoff MD This CT scan through the pancreas shows a mass in the neck associated with pancreatic duct dilatation and secondary atrophy in the pancreatic tail. These findings are consistent with a diagnosis of a primary carcinoma of the pancreas. Based on the desmoplastic nature of the process the tumor is most likely a scirrhous adenocarcinoma. 30101a05 Courtesy Ashley Davidoff MD
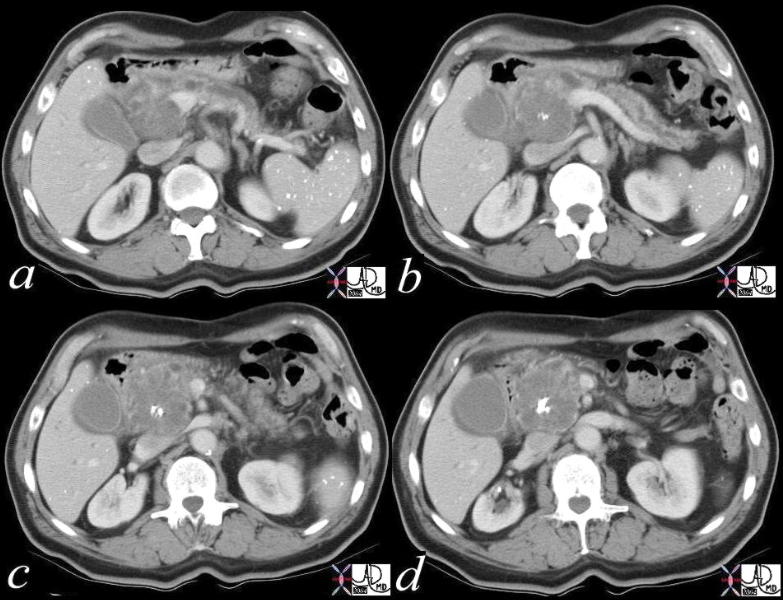
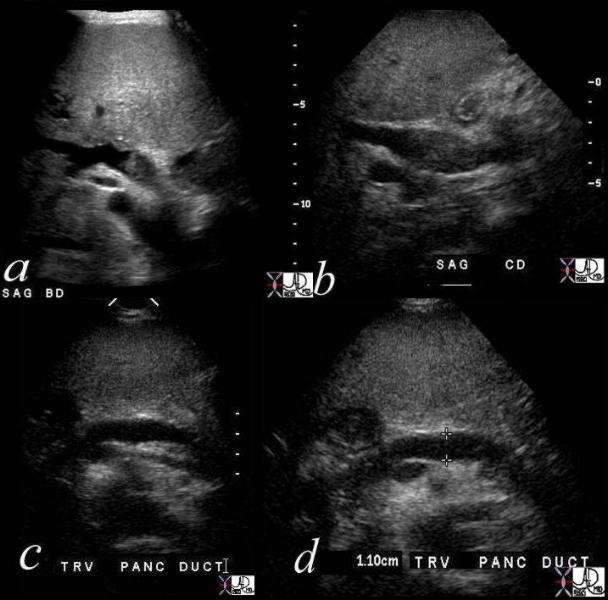
 This combination series of CTscans (a,b) and USscans (c,d) in a 23 year old female show a very large duct with secondary atrophy of the pancreatic parenchyma. When the duct is so large, it may be difficult to perceive the ductal origin of the abnormality. The cause of the dilated duct in this young patient was unusual, and although chronic pancreatitis is considered, her age went against the diagnosis. 40074c Courtesy Ashley Davidoff MD This combination series of CTscans (a,b) and USscans (c,d) in a 23 year old female show a very large duct with secondary atrophy of the pancreatic parenchyma. When the duct is so large, it may be difficult to perceive the ductal origin of the abnormality. The cause of the dilated duct in this young patient was unusual, and although chronic pancreatitis is considered, her age went against the diagnosis. 40074c Courtesy Ashley Davidoff MD
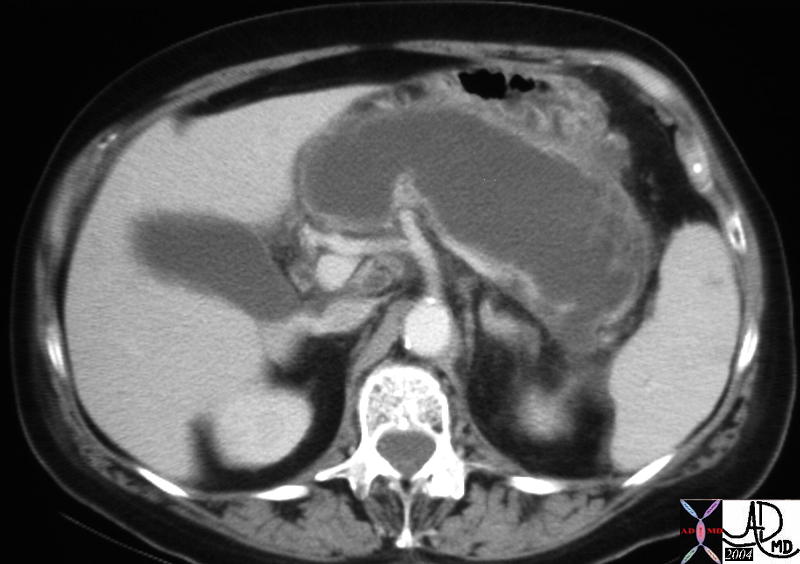 This CT scan through the pancreas shows a tubular cystic mass in the pancreatic body and tail, which conforms to the shape of the pancreatic tail and is associated with a thin rim of pancreatic tissue. The finding is consistent with an obstructed and dilated pancreatic duct with secondary pressure atrophy of the pancreas. The focal hypodensity in the spleen is of unknown significance. 40208 Courtesy Ashley Davidoff MD This CT scan through the pancreas shows a tubular cystic mass in the pancreatic body and tail, which conforms to the shape of the pancreatic tail and is associated with a thin rim of pancreatic tissue. The finding is consistent with an obstructed and dilated pancreatic duct with secondary pressure atrophy of the pancreas. The focal hypodensity in the spleen is of unknown significance. 40208 Courtesy Ashley Davidoff MD
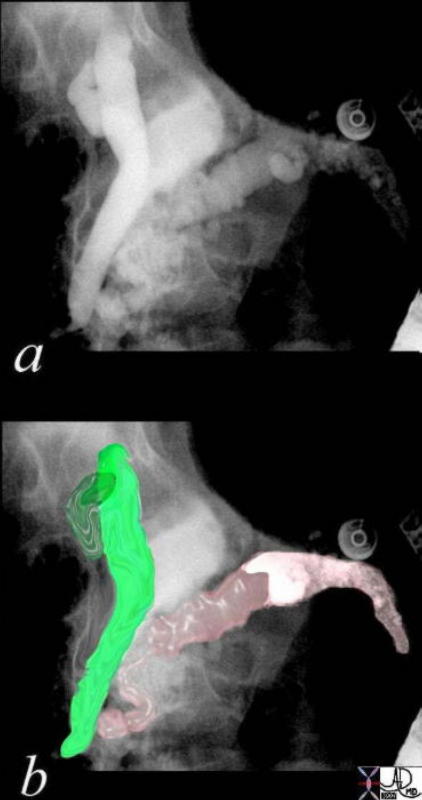
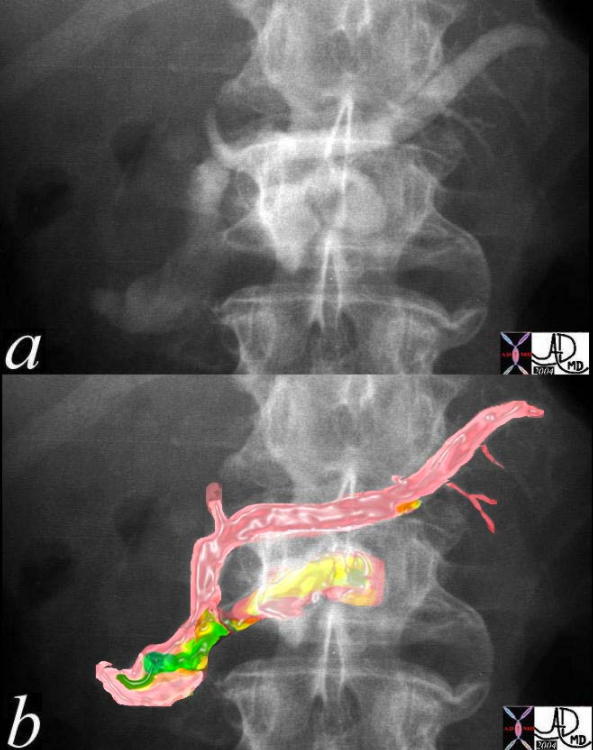 This ERCP reveals a mildly dilated pancreatic duct, being particularly prominent in the head and uncinate process. Filling defects as depicted in green in (b)are suggested. At ERCP the endoscopist noted excretion of mucus through the ampulla. These findings are consistent with a diagnosis of mucinous duct ectasia. 40517c0001 Courtesy Ashley Davidoff MD This ERCP reveals a mildly dilated pancreatic duct, being particularly prominent in the head and uncinate process. Filling defects as depicted in green in (b)are suggested. At ERCP the endoscopist noted excretion of mucus through the ampulla. These findings are consistent with a diagnosis of mucinous duct ectasia. 40517c0001 Courtesy Ashley Davidoff MD
The combination of images below reflects the changes of the above case in multimodality format.
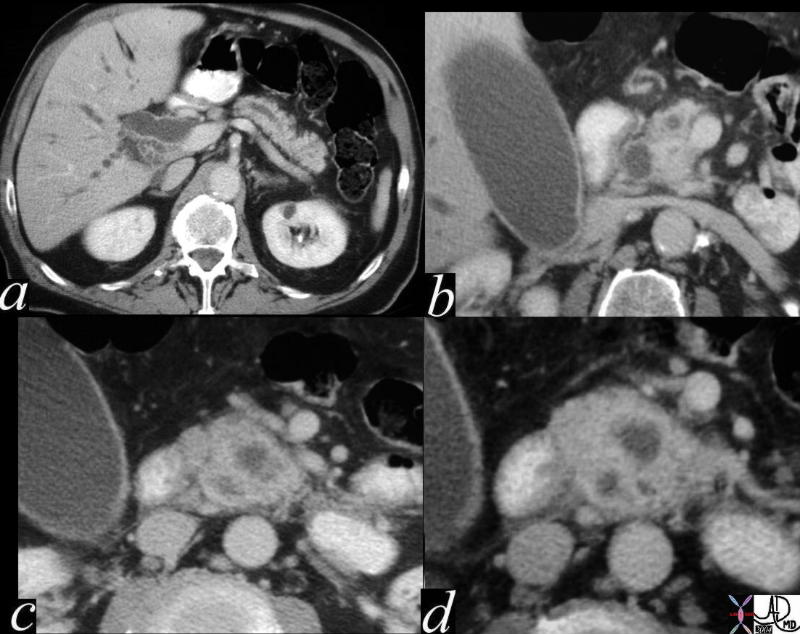 This CT scan series is of a patient with obstructive jaundice and shows a double duct sign suspicious for carcinoma off the head of the pancreas. A dilated pancreatic duct and a dilated CBD (“double duct” sign) is shown (a,b) and then 3 hypodensities and a rotund appearance of the head suggests an extra and unwanted component in the head of the pancreas. Can you identify the unwanted component from these images?. The findings nevertheless are consistent with a primary adenocarcinoma of the pancreas. 40840c01 Courtesy Ashley Davidoff MD This CT scan series is of a patient with obstructive jaundice and shows a double duct sign suspicious for carcinoma off the head of the pancreas. A dilated pancreatic duct and a dilated CBD (“double duct” sign) is shown (a,b) and then 3 hypodensities and a rotund appearance of the head suggests an extra and unwanted component in the head of the pancreas. Can you identify the unwanted component from these images?. The findings nevertheless are consistent with a primary adenocarcinoma of the pancreas. 40840c01 Courtesy Ashley Davidoff MD
Double Duct Sign
 This is a classical example of a double duct sign. The dilated pancreatic duct and bile duct almost point to the disease process in this image. A solid mass was identified in the head of the pancreas consistent with adenocarcinoma. 40837 Courtesy Ashley Davidoff MD This is a classical example of a double duct sign. The dilated pancreatic duct and bile duct almost point to the disease process in this image. A solid mass was identified in the head of the pancreas consistent with adenocarcinoma. 40837 Courtesy Ashley Davidoff MD
The combination of images below reflects the changes of the above case in at different levels and magnification.
This is a classical example of a “double duct” sign. The dilated pancreatic duct and bile duct in a, almost point to the disease process in this image. The mass was as predicted to be in the head of the pancreas. In c and d, a relatively small hypodense mass was identified whose scirrhous nature, and critical location caused early obstructive jaundice. 40840c01 Courtesy Ashley Davidoff MD
 This combination studies includes CTscans, MRIs, US scans, and an ERCP. They suggest a subtle mass in the head of the pancreas with early bile duct dilatation and more obvious pancreatic duct involvement. This was a case of adenocarcinoma of the head of the pancreas. 41293a16c Courtesy Ashley Davidoff MD This combination studies includes CTscans, MRIs, US scans, and an ERCP. They suggest a subtle mass in the head of the pancreas with early bile duct dilatation and more obvious pancreatic duct involvement. This was a case of adenocarcinoma of the head of the pancreas. 41293a16c Courtesy Ashley Davidoff MD
 A 57 year old female presents with jaundice. Her ERCP shows dilatation of the bile duct and pancreatic duct – the “double duct” sign characteristic of adenocarcinoma of the head of the pancreas. In this case the stricture appears quite distal. Chronic pancreatitis can also rarely cause the “double duct” sign. In this case an ampullary carcinoma was the cause explaining the distal position of the strictures. 04655c03 Courtesy Ashley Davidoff MD A 57 year old female presents with jaundice. Her ERCP shows dilatation of the bile duct and pancreatic duct – the “double duct” sign characteristic of adenocarcinoma of the head of the pancreas. In this case the stricture appears quite distal. Chronic pancreatitis can also rarely cause the “double duct” sign. In this case an ampullary carcinoma was the cause explaining the distal position of the strictures. 04655c03 Courtesy Ashley Davidoff MD
The combination of images below reflects the changes of the above case using a multimodality approach with pathological proof.
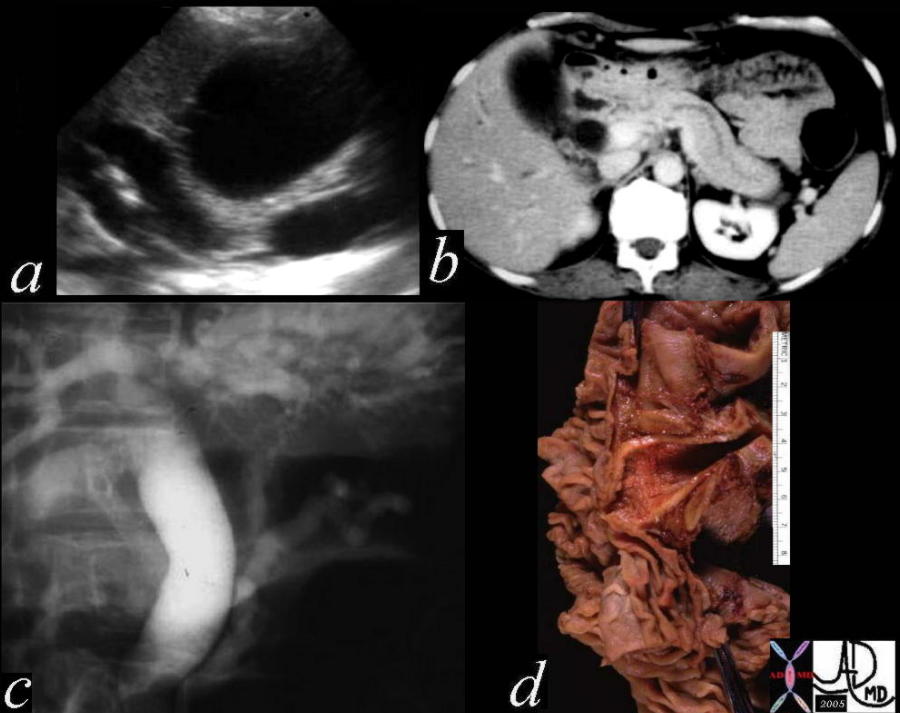 This is a series of images from the case history of a 57 year old female who presented with jaundice. The US image (a) shows a dilated bile duct and dilated pancreatic duct with no large mass between them. The CT shows a les impressive, but prominent pancreatic duct. The ERCP suggests a “double duct” sign. The pathology confirmed an ampullary carcinoma. 04655c05 Courtesy Ashley Davidoff MD This is a series of images from the case history of a 57 year old female who presented with jaundice. The US image (a) shows a dilated bile duct and dilated pancreatic duct with no large mass between them. The CT shows a les impressive, but prominent pancreatic duct. The ERCP suggests a “double duct” sign. The pathology confirmed an ampullary carcinoma. 04655c05 Courtesy Ashley Davidoff MD
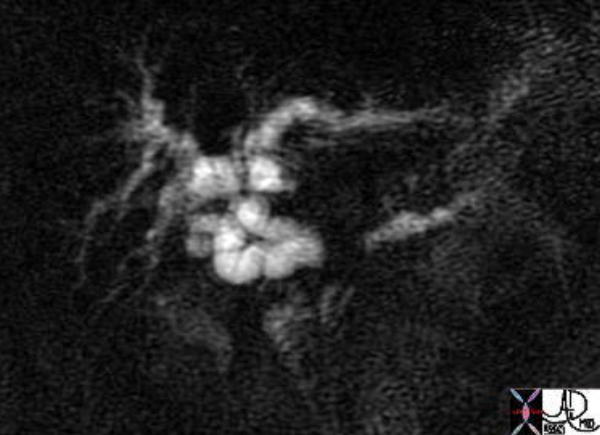 The image from an MRCP shows the MRI version of the double duct. The separation of the two ducts suggests a large size of the mass. This patient had pancreatic carcinoma. 41371 Courtesy of Ashley Davidoff MD The image from an MRCP shows the MRI version of the double duct. The separation of the two ducts suggests a large size of the mass. This patient had pancreatic carcinoma. 41371 Courtesy of Ashley Davidoff MD
The combination of images below reflects the changes of the above case at different levels. Cranially the liver is seen and caudally the pancreas is seen.
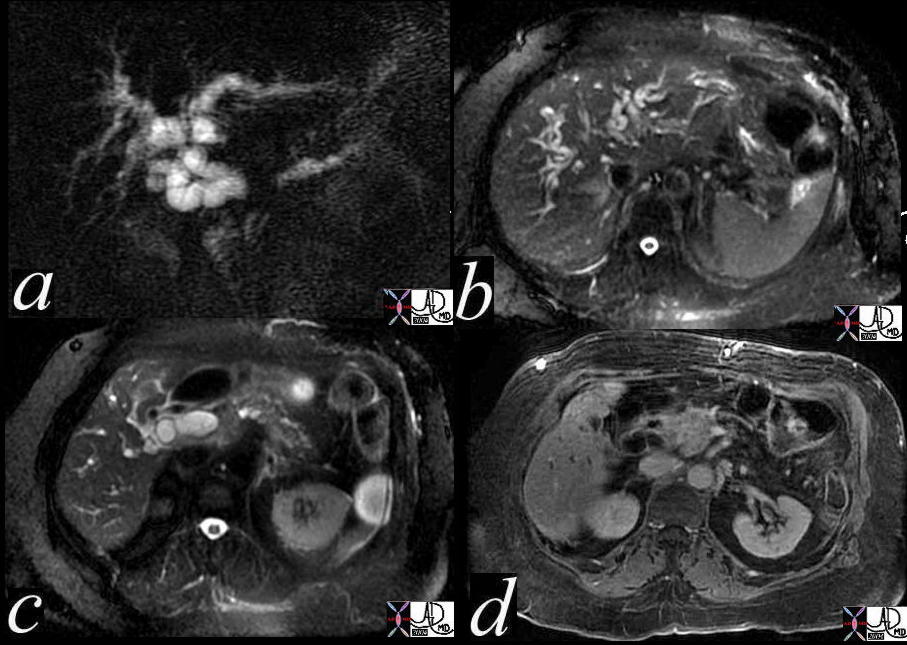 The image from an MRCP shows the MRI version of the “double duct” sign. The separation of the two ducts suggests a large size of the mass (a). Image b shows intrahepatic biliary dilatation, while image c shows CBD dilatation. Image d shows a mass in the head of the pancreas on the contrast enhanced sequence. This patient had pancreatic carcinoma. 41371c Courtesy of Ashley Davidoff MD The image from an MRCP shows the MRI version of the “double duct” sign. The separation of the two ducts suggests a large size of the mass (a). Image b shows intrahepatic biliary dilatation, while image c shows CBD dilatation. Image d shows a mass in the head of the pancreas on the contrast enhanced sequence. This patient had pancreatic carcinoma. 41371c Courtesy of Ashley Davidoff MD
 This CT study is a variation of the double duct sign. The biliary dilatation has been relieved by a stent while the pancreatic duct dilatation with secondary atrophy of the pancreas is quite apparent. This is a patient with pancreatic carcinoma.16312 Courtesy Ashley Davidoff MD This CT study is a variation of the double duct sign. The biliary dilatation has been relieved by a stent while the pancreatic duct dilatation with secondary atrophy of the pancreas is quite apparent. This is a patient with pancreatic carcinoma.16312 Courtesy Ashley Davidoff MD
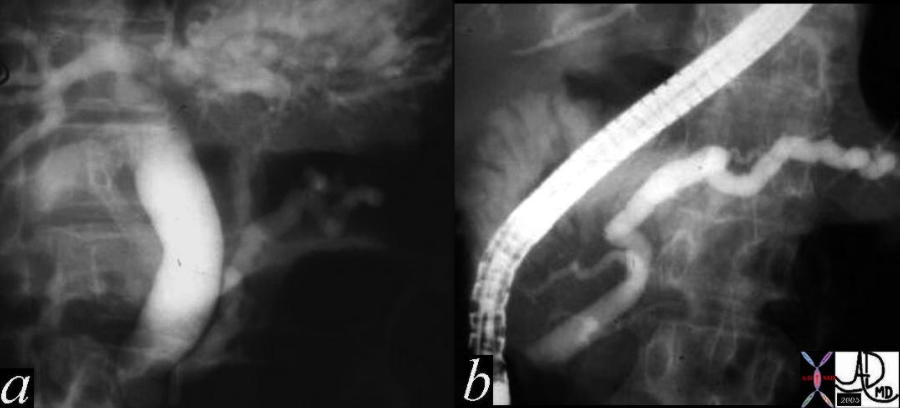
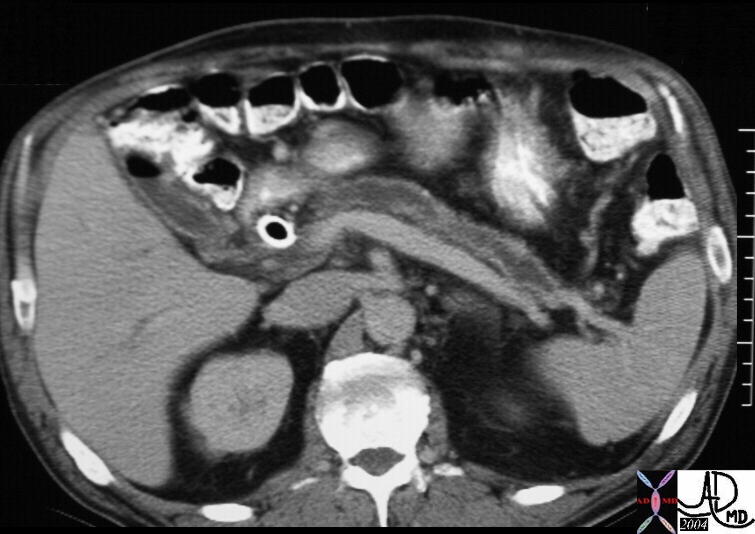
 At first glance this image from an ERCP looks like a double duct sign. In fact it does show that both ducts are dilated, but for different reasons other than cancer. The main pancreatic duct drains into the accessory duct of Santorini, while the CBD drains in usual fashion into the ampulla. This is a case of pancreas divisum. No pancreatic cancer was found on further workup. The etiology of the mild dilation is probably due to benign narrowing of both ducts at their insertion sites. 40615 Courtesy Ashley Davidoff MD At first glance this image from an ERCP looks like a double duct sign. In fact it does show that both ducts are dilated, but for different reasons other than cancer. The main pancreatic duct drains into the accessory duct of Santorini, while the CBD drains in usual fashion into the ampulla. This is a case of pancreas divisum. No pancreatic cancer was found on further workup. The etiology of the mild dilation is probably due to benign narrowing of both ducts at their insertion sites. 40615 Courtesy Ashley Davidoff MD
The combination of images below reflects the changes of the above case using a multimodality approach.
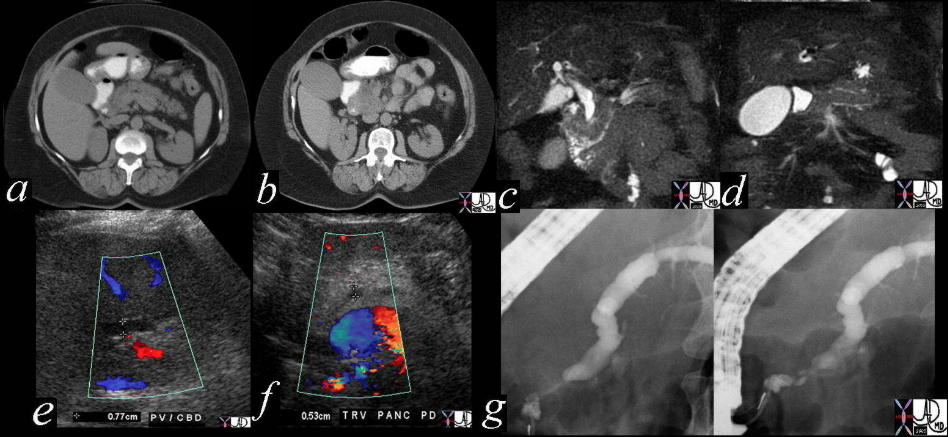
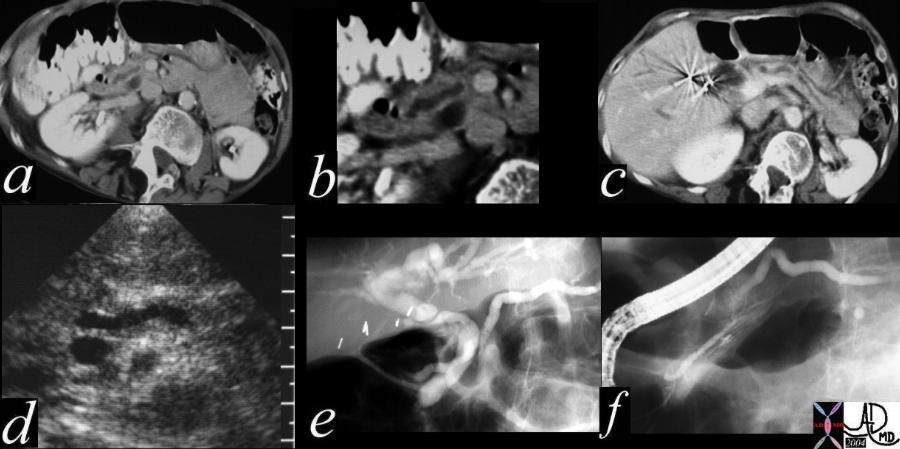 This combination series shows a dilated pancreatic duct in the head of the pancreas (a,b) as well as in the tail (c) The CBD is mildly dilated on US (d) The ERCP (e) shows that both ducts are dilated. At first glance a double duct sign seems likely since both ducts are dilated, but for different reasons. The main pancreatic duct drains into the accessory duct of Santorini, while the CBD drains in usual fashion into the ampulla. The smaller duct of Wirsung is seen mostly disconnected from the ductal system at large. This is a case of pancreas divisum. No pancreatic cancer was found on further workup 40617c01 Courtesy Ashley Davidoff MD This combination series shows a dilated pancreatic duct in the head of the pancreas (a,b) as well as in the tail (c) The CBD is mildly dilated on US (d) The ERCP (e) shows that both ducts are dilated. At first glance a double duct sign seems likely since both ducts are dilated, but for different reasons. The main pancreatic duct drains into the accessory duct of Santorini, while the CBD drains in usual fashion into the ampulla. The smaller duct of Wirsung is seen mostly disconnected from the ductal system at large. This is a case of pancreas divisum. No pancreatic cancer was found on further workup 40617c01 Courtesy Ashley Davidoff MD
 This is an ERCP showing a “double duct” sign. With the heavy intraductal calcification chronic alcoholic pancreatitis is definite. It is conceivable that the patient has a superimposed malignancy. In this case the double duct was caused by the strictures of chronic pancreatitis. 41245c06 Courtesy Ashley Davidoff MD This is an ERCP showing a “double duct” sign. With the heavy intraductal calcification chronic alcoholic pancreatitis is definite. It is conceivable that the patient has a superimposed malignancy. In this case the double duct was caused by the strictures of chronic pancreatitis. 41245c06 Courtesy Ashley Davidoff MD
 In this case we have a double duct sign as noted by US. The CBD is filled with sludge and pancreatic duct measures 11mm. This patient HIV positive and did not have pancreatic cancer. An HIV cholangiopathy, sludge impaction and infection involving both sites were considered. 41257c003 Courtesy Ashley Davidoff MD In this case we have a double duct sign as noted by US. The CBD is filled with sludge and pancreatic duct measures 11mm. This patient HIV positive and did not have pancreatic cancer. An HIV cholangiopathy, sludge impaction and infection involving both sites were considered. 41257c003 Courtesy Ashley Davidoff MD
|
 This is a CTscan of an 84 year old female patient in which a relatively small but normal size of the body of the pancreas is demonstrated. The duct is relatively prominent as a result of the involution of the glandular tissue, and is a normal finding. 43919 Courtesy Ashley Davidoff MD
This is a CTscan of an 84 year old female patient in which a relatively small but normal size of the body of the pancreas is demonstrated. The duct is relatively prominent as a result of the involution of the glandular tissue, and is a normal finding. 43919 Courtesy Ashley Davidoff MD In this elderly patient the enhanced MRI shows a prominent but normal pancreatic duct. 19955 Courtesy Ashley Davidoff MD
In this elderly patient the enhanced MRI shows a prominent but normal pancreatic duct. 19955 Courtesy Ashley Davidoff MD This ERCP demonstrates an enlarged main pancreatic duct. The duct should normally measure only 2-5 mms. The scope size is usually 10mm in diameter and in this case the duct is more than half that size. The cause of the ductal dilatation in this patient is not known. A prominent duct of Santorini appears to originate off the main duct. 04184 Courtesy Ashley Davidoff MD
This ERCP demonstrates an enlarged main pancreatic duct. The duct should normally measure only 2-5 mms. The scope size is usually 10mm in diameter and in this case the duct is more than half that size. The cause of the ductal dilatation in this patient is not known. A prominent duct of Santorini appears to originate off the main duct. 04184 Courtesy Ashley Davidoff MD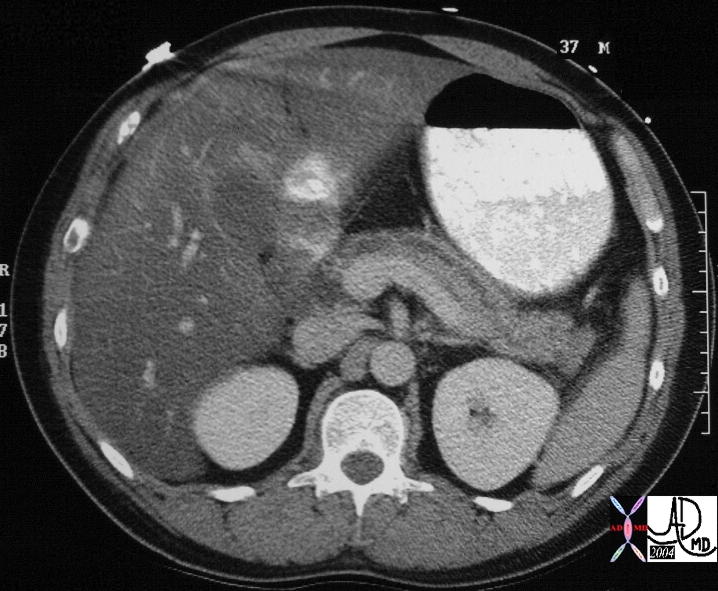 This CT scan is from a 37 year old male showing a duct that appears to be mildly enlarged. In many instances, enlargement is a subjective interpretation. Electronic and manual measurement at this size can be inaccurate. Associated severe fatty change of the liver is noted. 28946 Courtesy Ashley Davidoff MD
This CT scan is from a 37 year old male showing a duct that appears to be mildly enlarged. In many instances, enlargement is a subjective interpretation. Electronic and manual measurement at this size can be inaccurate. Associated severe fatty change of the liver is noted. 28946 Courtesy Ashley Davidoff MD