The Common Vein copyright 2008
Alok Anand
Definition
Gallstone pancreatitis is an inflammatory diseaseof the pancreas and caused by the passage of gallstones into the common bile duct and is the most common cause of pancreatitis in the elderly non alcoholic population in developed countries.
This condition can result in hemorrhage, edema, and necrosis of the pancreas. This disease can have widespread effects as well, leading to systemic inflammatory response syndrome with shock, organ failure, and possibly death.
Structurally this disease entity reflects a mechanical blockage of the outflow of the exocrine portion of the pancreas. As the pancreas is intimately involved with digestion, the progression of this disease can cause edematous changes of the pancreas and biliary tract, as well as hemorrhage into the abdomen. Later, it can cause pseudocysts to form around the pancreas.
The functional consequences of gallstone pancreatitis reflect the high density of digestive enzymes produced in the pancreas. Normally, enzymatic proteins in the form of zymogens (inactivated proteins) are released in granules from the pancreas, when they enter the digestive tract, these enzymes become activated and can safely break apart food contents. When the flow of these enzymes is blocked, they can become activated within the bile ducts, and begin to degrade the ducts, as well as the pancreatic parenchyma. This leads to the damage and inflammation of the organ and surrounding tissues.
Patients present clinically with dull abdominal pain of increasing intensity, usually in the epigastric area. Fever and tachycardia, along with nausea and vomiting are common. Pain is typically improved when patients are supine. Some patients may exhibit jaundice. If ascending cholangitis is present, the classic finding are, RUQ pain, jaundice, fever/elevated white cell count, also known as Charcot’s triad. The additional presence of hypotension, and mental status change comprise another eponymous constellation known as Raynaud’s pentad.
Pancreatitis is diagnosed clinically, though laboratory tests and imaging are used to support a working diagnosis. Serum amylase and lipase levels are elevated, as well liver enzymes, alkaline phosphatase, and bilirubin, due to gallstones. Imaging of pancreatitis is initially through ultrasonography to evaluate the biliary tree for the presence of gallstones. MRCP may also be used for this. Abdominal CT, though generally not indicated in mild cases, is useful in evaluating complications of severe pancreatitis. The degree of pancreatitis can be graded using Balthazar’s scale:
A – Normal
B – Enlargement
C – Peripancreatic inflammation
D – Single fluid collection
E – Multiple fluid collections
Mortality risk is evaluated using Ranson’s criteria, which look at various factors on admission and after 48 hours.
This condition is treated with aggressive IV hydration with nothing taken by mouth, antibiotics, and close observation for decompensation. Surgical intervention depends on structural changes, such as damage to the ductal system. If infected necrosis is present, percutaneous drainage may be used. Further, if pseudocysts develop, they should be watched for 6 weeks before attempting surgery. Once pain and poor appetite improve, introducing food with high protein content is recommended. Pain management is another important consideration, and generally morphine should be avoided as it can cause spasm of the spincter of Oddi.
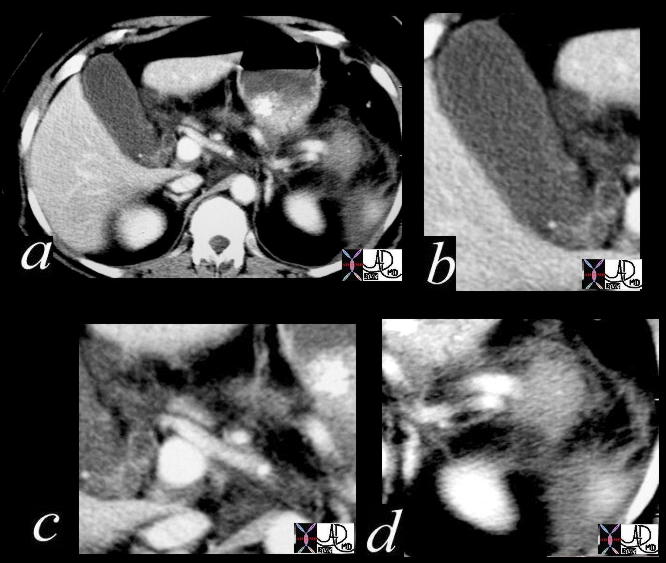 Gallstone Pancreatitis Gallstone Pancreatitis |
| 16225a01c Courtesy Ashley DAvidoff MD code gallbladder + infundibulum fx calcification dx cholelithiasis code cystic duct fx dilated fx enhancingwall dx obstruction code abdomen retroperitoneum Gerota’s fascia fx indurated dx gallstone pancreatitis + imaging radiology CTscan |
 Gallstone Pancreatitis – Pancreatic Necrosis Gallstone Pancreatitis – Pancreatic Necrosis |
| 05265 Courtesy Ashley Davidoff MD code pancreas fx air fx fluid cystic fx mass dx necrotizing pancreatitis code gallbladder fx stones dx cholelithiasis code lung pleura fx effusion dx sympathetic effusion dx gallstone pancreatitis complicated by gangrene necrosis possible infection imaging radiology CTscan code acute inflammation |